

ABSTRACT
Chronic kidney disease (CKD) is a prevalent complication of Type II diabetes (T2D). The coexistence of CKD with T2D is comparable to cardiovascular disease (CVD) when the estimated glomerular filtration rate declines below 60 ml/min/1.73 m2. Screening and early detection of people with high risk for CKD would be beneficial in managing CKD progress and the associated complications such as CV complications. Renin-angiotensin-aldosterone system inhibitors (RAASi) have demonstrated beneficial effects in delaying CKD progression, but they carry the risk of hyperkalemia. Nonsteroidal mineralocorticoid antagonists (nsMRA), such as finerenone, exhibit considerable efficacy in their anti-inflammatory, antifibrotic, and renal protective effects with demonstrable reductions in CV complications. In addition, nsMRAs do not cause significant changes in serum potassium levels compared to traditional steroidal MRA. Ongoing research explores the capacity of the sodium-glucose transport protein 2 inhibitors (SGLT-2i), combined with nsMRA, to produce synergistic renal protective effects and reduce the risk of hyperkalemia. Also, a dedicated renal outcomes study (FLOW study) involving a once-weekly injectable Glucagon-like peptide-1 receptor agonist, semaglutide, was halted early by the data monitoring committee due to having achieved the predefined efficacy endpoint and considerations related to renal disease. In CKD patients with T2D on nsMRA, hyperkalemia management requires a comprehensive approach involving lifestyle adjustments, dietary modifications, regular serum potassium level monitoring, and potassium binders, if necessary. Withholding or down-titration of nsMRAs with close monitoring of serum potassium levels may be required in patients with concerning potassium levels. In light of the current state of knowledge, this review article explores the perspectives and approaches that HCPs may consider when monitoring and managing hyperkalemia in CKD patients with T2D.
Plain Language Summary
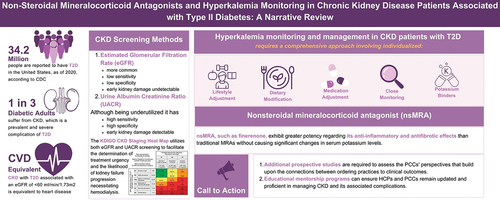
Chronic Kidney Disease (CKD) is a common and serious problem among people with Type II Diabetes (T2D). People who have CKD with T2D are at a higher risk for heart disease after normal kidney function declines below certain levels. Renin-angiotensin-aldosterone system inhibitors are a group of medications that can help delay CKD progression but may cause a rise in circulating potassium levels. Nonsteroidal mineralocorticoid antagonist (nsMRA), such as finerenone, can reduce kidney inflammation and damage, with noted cardiovascular benefits, and with less effect on serum potassium levels as compared to their steroid-based counterparts. Researchers are studying whether combining blood sugar medications such as sodium-glucose transport protein-2 inhibitors (SGLT-2i) and finerenone can help protect the kidneys and heart. They also want to see if this combination can prevent high potassium levels. This article talks about ways to check and monitor potassium levels in CKD patients with T2D who may be taking nsMRA. To manage high potassium levels in people with CKD and T2D, doctors may suggest lifestyle changes, dietary adjustments, potassium-lowering medication, or adjustment of other medications with close monitoring of potassium levels.
Graphical Abstract
Declaration of financial/other relationships
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. Peer reviewers on this manuscript have received an honorarium from IPGM for their review work but have no other relevant financial relationships to disclose.
Acknowledgments
The authors would like to acknowledge the medical writing support provided by Mahmoud Azqul of ILM Consulting Services, LLC., which was funded by Bayer US, LLC. The authors would also like to acknowledge the editorial support, visualization and graphical abstract development provided by Aqsa Dar of ILM Consulting Services, LLC., which was also funded by Bayer US, LLC. ILM’s services complied with international guidelines for Good Publication Practice (GPP 2023).
Author contributions
All authors contributed to the writing and reviewing of each draft and reviewing and approving the final draft for submission. Javier Morales: Conceptualization, Writing – review & editing. Biff F. Palmer: Conceptualization, Writing – review & editing.