

Abstract
Background
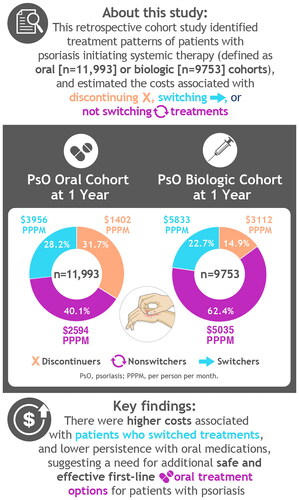
Psoriasis is a chronic, immune-mediated, systemic inflammatory disorder associated with high costs. This study evaluated real-world treatment patterns and associated costs in patients in the United States with psoriasis initiating systemic oral or biologic treatments.
Methods
This retrospective cohort study used IBM® (now Merative™) MarketScan® Commercial and Medicare claims (1 January 2006–31 December 2019) to evaluate patterns of switching, discontinuation, and nonswitching in two cohorts of patients initiating oral or biologic systemic therapy. Total pre-switch and post-switch costs were reported per-patient per-month (PPPM).
Results
Each cohort was analyzed (oral, n = 11,993; biologic; n = 9753). Among the oral and biologic cohorts, 32% and 15% discontinued index and any systemic treatment within 1 year of initiation; 40% and 62% remained on index therapy; and 28% and 23% switched treatment, respectively. In the oral and biologic cohorts, total PPPM costs within 1 year of initiation for nonswitchers, patients who discontinued, and patients who switched were $2594, $1402, and $3956, respectively, and $5035, $3112, and $5833, respectively.
Conclusion
This study identified lower persistence in the oral treatment cohort, higher costs associated with switching, and a need for safe and effective oral treatment options for patients with psoriasis to delay the switch to biologic therapy.
Graphical Abstract
Acknowledgments
The authors thank Ann Wang, MA, of Bristol Myers Squibb for assistance with data analysis and results interpretation. Medical writing and editorial assistance was provided by Nicole Boyer, PhD, MPH, of Peloton Advantage, LLC, an OPEN Health company, and funded by Bristol Myers Squibb.
Disclosure statement
J.Z., Y.Z., Q.X., Y.B., and D.D. are employees and shareholders of Bristol Myers Squibb. X.C. was an employee and shareholder of Bristol Myers Squibb at the time of the study. S.T. was completing a fellowship in Worldwide Health Economics and Outcomes Research at Bristol Myers Squibb at the time of the study. L.P. is an employee of Mu Sigma, which has received consulting fees from Bristol Myers Squibb. J.J.W. is or has been an investigator, consultant, or speaker for AbbVie, Almirall, Amgen, Arcutis, Aristea Therapeutics, Bausch Health, Boehringer Ingelheim, Bristol Myers Squibb, Dermavant, DermTech, Dr. Reddy’s Laboratories, Eli Lilly, EPI Health, Galderma, Janssen, LEO Pharma, Mindera Health, Novartis, Pfizer, Regeneron, Samsung Bioepis, Sanofi Genzyme, Solius, Sun Pharmaceutical, UCB, and Zerigo Health.
Data availability statement
The Bristol Myers Squibb policy on data sharing may be found at https://www.bms.com/researchers-and-partners/independent-research/data-sharing-request-process.html.