

Abstract
Introduction
Intraamniotic infection (IAI) and subsequent early-onset neonatal sepsis (EONS) are among the main complications associated with preterm prelabor rupture of membranes (PPROM). Currently used diagnostic tools have been shown to have poor diagnostic performance for IAI. This study aimed to investigate whether the exposure to IAI before delivery is associated with short-term variation of the fetal heart rate in pregnancies with PPROM.
Methods
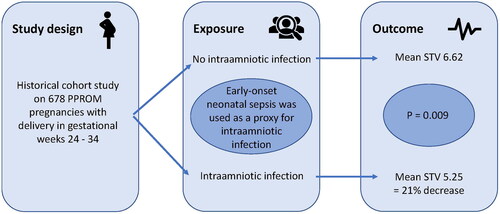
Observational cohort study of 678 pregnancies with PPROM, delivering between 24 + 0 and 33 + 6 gestational weeks from 2012 to 2019 in five labor units in Stockholm County, Sweden. Electronic medical records were examined to obtain background and exposure data. For the exposure IAI, we used the later diagnosis of EONS in the offspring as a proxy. EONS is strongly associated to IAI and was considered a better proxy for IAI than the histological diagnosis of acute chorioamnionitis, since acute chorioamnionitis can be observed in the absence of both positive microbiology and biochemical markers for inflammation. Cardiotocography traces were analyzed by a computerized algorithm for short-term variation of the fetal heart rate, which was the main outcome measure.
Results
Twenty-seven pregnancies were categorized as having an IAI, based on the proxy diagnosis of EONS after birth. Fetuses exposed to IAI had significantly lower short-term variation values in the last cardiotocography trace before birth than fetuses who were not exposed (5.25 vs 6.62 ms; unadjusted difference: −1.37, p = 0.009). After adjustment for smoking and diabetes, this difference remained significant. IAI with a later positive blood culture in the neonate (n = 12) showed an even larger absolute difference in STV (−1.65; p = 0.034), with a relative decrease of 23.5%.
Conclusion
In pregnancies with PPROM, fetuses exposed to IAI with EONS as a proxy have lower short-term variation of the fetal heart rate than fetuses who are not exposed. Short-term variation might be useful as adjunct surveillance in pregnancies with PPROM.
GRAPHICAL ABSTRACT
Acknowledgments
We thank Thomas Andersson for his important statistical input and work. We thank Viveka Nordberg who is a neonatologist, and Nikos Papadogiannakis who is a perinatal pathologist, for helpful input and discussion regarding the validation of data and diagnoses of EONS, HCA and FIR. We thank Ellen Knapp, PhD, from Edanz (https://edanz.com/ac) for editing a draft of this manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
The participants of this study did not give written consent for their data to be shared publicly, so due to the sensitive nature of the research supporting data is not available.