

Abstract
Background
Oral corticosteroids (OCS) are often prescribed for chronic obstructive pulmonary disease (COPD) exacerbations.
Methods
This observational, individually matched historical cohort study used electronic medical records (1987–2019) from the UK Clinical Practice Research Datalink linked to English Hospital Episode Statistics (HES) to evaluate adverse outcomes in patients with COPD who used OCS (OCS cohort) and those not exposed to OCS (non-OCS cohort). Risk of 17 adverse outcomes was estimated using proportional hazard regression.
Results
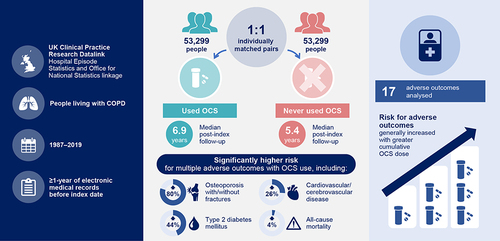
Of 323,722 patients, 106,775 (33.0%) had COPD-related OCS prescriptions. Of the 106,775 patients in the overall cohort, 58,955 had HES linkage and were eligible for inclusion in the OCS cohort. The individual matching process identified 53,299 pairs of patients to form the OCS and non-OCS cohorts. Median follow-up post-index was 6.9 years (OCS cohort) and 5.4 years (non-OCS cohort). Adjusted risk of multiple adverse outcomes was higher for the OCS cohort versus the non-OCS cohort, including osteoporosis with/without fractures (adjusted hazard ratio [aHR] 1.80; 95% confidence interval [CI] 1.70–1.92), type 2 diabetes mellitus (aHR 1.44; 95% CI 1.37–1.51), cardiovascular/cerebrovascular disease (aHR 1.26; 95% CI 1.21–1.30), and all-cause mortality (aHR 1.04; 95% CI 1.02–1.07). In the OCS cohort, risk of most adverse outcomes increased with increasing categorized cumulative OCS dose. For example, risk of cardiovascular/cerebrovascular disease was 34% higher in the 1.0–<2.5 g group versus the <0.5 g group (HR 1.34; 95% CI 1.26–1.42).
Conclusion
Any OCS use was associated with higher risk of adverse outcomes in patients with COPD, with risk generally increasing with greater cumulative OCS dose.
Plain Language Summary
Many patients with chronic obstructive pulmonary disease (COPD) have occasions when their symptoms suddenly worsen, called flare-ups or exacerbations. To treat flare-ups, doctors might prescribe a course of steroid tablets (oral corticosteroids or OCS for short). Doctors might also prescribe “rescue packs” containing OCS and antibiotics, to keep at home and start taking when needed.
While OCS may speed up recovery from flare-ups, repeated use may have negative health effects. We studied effects of OCS use in patients with COPD, using anonymized electronic patient medical records in England. These databases are made available following a high-quality research proposal to research and ethics committees.
Of 323,722 patients with COPD, around one-third received OCS for flare-ups. We studied 17 outcomes including important medical diagnoses and death. We grouped patients into 53,299 pairs so that every patient who used OCS matched a similar patient (eg, the same age and sex) who never used OCS. The patients were followed for an average of 6.9 years (used OCS) and 5.4 years (never used OCS).
Most diagnoses, including diabetes, osteoporosis, cardiovascular/cerebrovascular disease, and death, were more likely in patients who used OCS than those who never used OCS. Patients using larger amounts of OCS over time were generally more likely to experience diagnoses or die.
These results show risks of using OCS, even occasionally, in patients with COPD. Flare-up prevention is important, for example with appropriate daily “maintenance” medication, vaccinations for infections, and quitting smoking, thereby reducing health effects from OCS use for flare-ups.
Graphical Abstract
Data Sharing Statement
Per the Clinical Practice Research Datalink Independent Scientific Advisory Committee guidance, the data will not be made available for sharing.
Ethical Approval
The study protocol was approved by the CPRD Independent Scientific Advisory Committee (reference number 20_159R), and the study was registered with the European Network of Centres for Pharmacoepidemiology and Pharmacovigilance (ENCePP; EUPAS35975). No patient-identifying information was accessible during the study.
Acknowledgments
The authors thank Hilda de Jong, PhD (the PHARMO Institute, Utrecht, the Netherlands) for her assistance in developing the study protocol. The authors also thank Sharen Lee (Cardiovascular Analytics Group, Hong Kong) for her technical assistance in generating figures for the dose-dependent relationship between OCS dose and adverse outcomes. The authors also thank Colin Bonner, Linda Stotsky, Mario Marinazzo, and Philomena Britto, for their review of the plain language summary as people living with COPD; these individuals were compensated for their time. Medical writing support, under the guidance of the authors, was provided by Sara Cameron, MPhil, and Sarah Piggott, MChem, CMC Connect, a division of IPG Health Medical Communications, funded by AstraZeneca, in accordance with Good Publication Practice (GPP 2022) guidelines.Citation46
Author Contributions
All authors made a significant contribution to the work reported. DP and VC contributed to study conception or design, data acquisition, data analysis, and data interpretation. MB and AP contributed to data interpretation. GT, CA, and JZ contributed to data analysis and data interpretation. DS contributed to data acquisition, data analysis, and data interpretation. XX, HM, and BE contributed to study conception or design and data interpretation. All authors took part in drafting, revising, or critically reviewing the article, gave final approval for the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
GT and CA are former employees of the Observational and Pragmatic Research Institute (OPRI), which was funded by AstraZeneca to conduct this study. VC, JZ, and DS are employees of OPRI, which was funded by AstraZeneca to conduct this study. BE, XX, and HM are employees of AstraZeneca and hold stock and/or stock options in the company. MB has received research grants to her institution from AstraZeneca; honoraria to her institution from AstraZeneca, Chiesi, and GlaxoSmithKline; and is an advisory board member for Albus Health and ProAxsis. AP has received scientific grants to his institution from Agenzia Italiana del Farmaco (AIFA), AstraZeneca, Chiesi, GlaxoSmithKline, and Sanofi; has received consulting fees from AstraZeneca, Avillion, Chiesi, ELPEN Pharmaceuticals, GlaxoSmithKline, Novartis, and Sanofi; has received payment or honoraria for lectures, presentations, speaker bureaus, or educational events from AstraZeneca, Avillion, Chiesi, Edmond Pharma, ELPEN Pharmaceuticals, Moderna, GlaxoSmithKline, IQVIA, Menarini, Mundipharma, Novartis, Sanofi, and Zambon; and is an advisory board member for AstraZeneca, Avillion, Chiesi, ELPEN Pharmaceuticals, GlaxoSmithKline, IQVIA, MSD, Novartis, and Sanofi. DP is an employee of OPRI, which was funded by AstraZeneca to conduct this study; has advisory board membership with AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Sanofi Genzyme, and Thermo Fisher; has consultancy agreements with Airway Vista Secretariat, AstraZeneca, Boehringer Ingelheim, Chiesi, EPG Communication Holdings Ltd, FIECON, Fieldwork International, GlaxoSmithKline, Mundipharma, Mylan, Novartis, OM Pharma SA, PeerVoice, Phadia AB, Spirosure Inc, Strategic North Limited, Synapse Research Management Partners S.L., Talos Health Solutions, Theravance, and WebMD Global LLC; has received grants and unrestricted funding for investigator-initiated studies (conducted through OPRI) from AstraZeneca, Boehringer Ingelheim, Chiesi, Mylan, Novartis, Regeneron Pharmaceuticals, Respiratory Effectiveness Group, Sanofi Genzyme, Theravance, and UK National Health Service; has received payment for lectures/speaking engagements from AstraZeneca, Boehringer Ingelheim, Chiesi, Cipla, GlaxoSmithKline, Kyorin, Mundipharma, Mylan, Novartis, Regeneron Pharmaceuticals, and Sanofi Genzyme; has received payment for travel/accommodation/meeting expenses from AstraZeneca, Boehringer Ingelheim, Mundipharma, Mylan, Novartis, and Thermo Fisher; has stock/stock options from AKL Research and Development Ltd, which produces phytopharmaceuticals; owns 74% of the social enterprise Optimum Patient Care Ltd (Australia and UK) and 92.61% of OPRI (Singapore); has a 5% shareholding in Timestamp, which develops adherence monitoring technology; is peer reviewer for grant committees of the UK Efficacy and Mechanism Evaluation Programme and Health Technology Assessment; and has been an expert witness for GlaxoSmithKline. The authors report no other conflicts of interest in this work.