Figures & data
Table 1 Distribution of patients according to location of the tumour.
Table 2 Distribution of patients according to initial TNM staging.
Table 3 Distribution and initial specific staging of patients with ano-rectal tumors.
Table 4 Distribution of patients according to initial status of sphincteric mechanism.
Table 5 Distribution of patients according to MRI detailed characteristics of positive MRF involvement.
Fig. 1 (Initial MRI study): A 62 years old male patient presented with bleeding per rectum and the PR examination revealed a rectal mass. MRI study with rectal distension using sonographic gel; (a) and (b) Sagittal high resolution T2WIs showing the lower rectal mass lesion (red arrows) about 3.5 cm from the anal verge. (c) and (d) Axial high resolution T2WIs showing the rectal mass with intermediate signal intensity extending from 9 to 3o'clock, no extension beyond the muscularis propria with implication of the internal sphincter from 11 to 1o'clock (green arrow). (e) Coronal high resolution T2WI showing extension 8 mm below puborectalis sling. (f) ADC map showing hypointense signal of the rectal mass denoting restricted diffusion (0.8 × 10−3 mm2/s). The preliminary imaging based staging was c T2 N0.
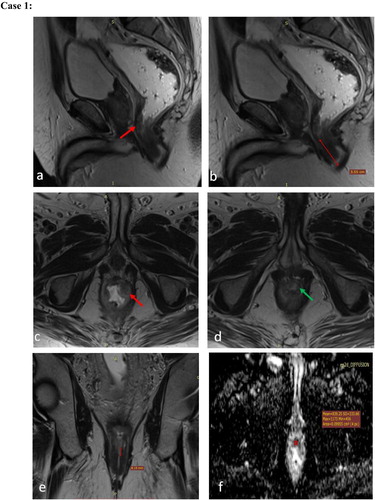
Fig. 2 (Post-neoadjuvant therapy MRI study): for the same patient after 5?months showed a non-responding lower rectal mass lesion with same tissue characteristics at T2WI and ADC maps, same dimensions and distal resectability features; resulting in TRG 5 and imaging based staging yc T2N0. Post CRT MRI study. (a) Sagittal high resolution T2WI and (b) ADC map showing the lower rectal mass lesion with the intermediate T2 signal (red arrow in a) and ADC values about 0.8?×?10−3?mm2/s denoting restricted diffusion. The patient performed abdominoperineal resection with the post-operative histopathology revealed a moderately differentiated rectal adenocarcinoma, 10 out of 10 nodes excised was free, margins free.
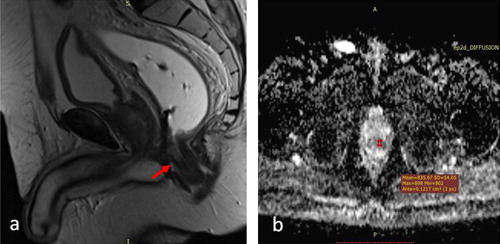
Fig. 3 (Initial MRI study): A 66?years old male patient diagnosed as rectal mass and referred from the oncology department for initial staging. MRI study; (a) and (b) Sagittal high resolution T2WIs, (c) and (d) axial high resolution T2WIs, (e) Coronal and (f) Axial high resolution T2WIs, (g) and (h) DWI and ADC maps showing a low third rectal mass lesion with intermediate SI, about 2.7?cm from the anal verge, crossing the puborectal sling by 7?mm, involving the four quadrants circumferentially with focal interruption of the musculosa at 9o'clock (red arrow in c) and implication of the upper 7?mm of the internal sphincters from 11 to 1o'clock (green arrows in d). An extramesorectal regional right internal iliac suspicious node is noted (blue arrow in f). Resticted diffusion was noted at DWI with ADC values about 0.8?×?10−3?mm2/s. The preliminary imaging based staging is cT3a (below APR, CRM−ve) Nx, stage 2 anal complex invasion.
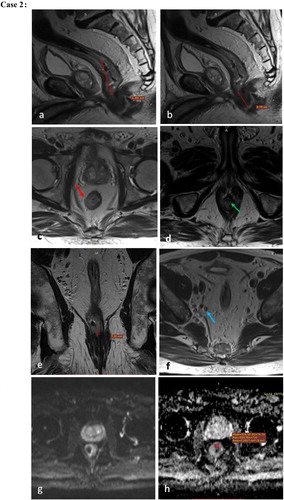
Fig. 4 (Post-neoadjuvant therapy MRI study): after 4?months revealed marked therapeutic Response (TRG?=?2: Dense fibrosis with absent or minimal residual disease). Spared sphincters. The preliminary imaging based staging is yc T0-2N0. MRI study with rectal distension using sonographic gel. (a) Sagittal high resolution T2WI, (b) and (d) Axial high resolution T2WIs, (c) Coronal high resolution T2WI, (e) and (f) DWI and ADC maps showing the lower third rectal lesion currently displaying low SI at T2WI denoting fibrosis, 6?cm from the anal verge, involving three quadrants circumferentially (red arrow in b) with no implication of the anal sphincteric complex (best depicted in c). The pathologically enlarged nodes. DWI showed no restriction. The patient performed low anterior resection (LAR) with the histopathology revealed moderately differentiated rectal adenocarcinoma, Mandrad grade 2 with 7 out of 7 nodes excised free, margins free and donuts free.
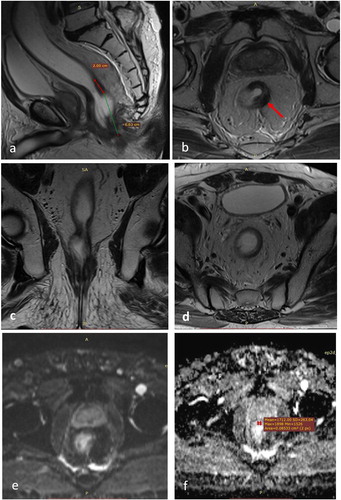
Fig. 5 (Initial MRI study): A 67?years old male patient presented with bleeding per rectum and diagnosed as rectal mass by endoscopy. Initial MRI study; (a) and (b) Sagittal high resolution T2WI, (c) and (d) axial high resolution T2WI, (e) and (f) DWI and ADC maps showing an upper rectal mass lesion, opposite to the spared APR (yellow arrow in b), about 3?cm in maximum length, 10.8?cm from the anal verge and 5.6?cm from the puborectalis sling, extending circumferentially from 7 to 12o'clock with 4?mm extramural depth of invasion (EMDI) beyond the muscularis propria into mesorectal fat. Restricted diffusion is seen in DWI with hyperintense signal and ADC values about 0.8?×?10−3?mm2/s. The preliminary imaging based staging is c T3b Nx. Opposite to APR and CRM spared.
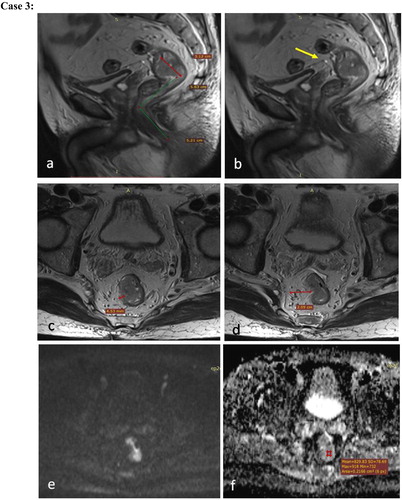
Fig. 6 (Post-neoadjuvant therapy MRI study): The post-neoadjuvant CRT MRI study after 4?months revealed partially responding upper third rectal neoplasm (TRG?=?3). The preliminary imaging based staging is yc T1 or T2 N0. Post neoadjuvant MRI study; (a) and (b) Sagittal and axial high resolution T2WI respectively, (c) and (d) DWI and ADC maps showing the previously noted upper rectal mass lesion, currently regressed in size about 2?cm in maximum length and 8.7?mm in maximum thickness, extending from circumferentially from 7 to 9o'clock with no evident of EMDI at current study, foci of restricted diffusion was seen with ADC values about 0.8?×?10−3?mm2/s. The patient performed left hemicolectomy with low anterior resection. The post-operative histopathology revealed moderately differentiated rectal adenocarcinoma, with 14 out of 14 nodes excised were free, margins free.

Fig. 7 (Initial MRI study): A 51?years old female patient diagnosed as rectal mass and referred from the oncology department for initial staging. Initial MRI with rectal distension using sonographic gel. (a) Sagittal high resolution T2WI, (b), (c) and (e) Axial high resolution T2WI, (d), (f) Coronal high resolution T2WI, (g) and (h) DWI and ADC maps showing an upper rectal mass lesion, about 5?cm in maximum length, 10?cm from the anal verge, showing intermediate signal intensity with involvement of the four quadrant of the rectal wall circumferentially. EMDI is noted all around the rectal wall with about 2?mm from the MRF at 8o'clock (red arrow in b). Suspected EMVI is noted at 9o'clock (yellow arrow in c). Multiple mesorectal adenopathies were seen (blue arrow in c, d, e) around the tumor and averaging 6?mm in size with some abutting the mesorectal fascia (red arrow in e). Inferior mesenteric extramesorectal regional node was seen, averaging 7?mm im size (green arrow in f). Restricted diffusion noted with ADC about 0.8?×?10−3?mm2/s. Preliminary imaging based staging is c T3c N2b (CRM+).
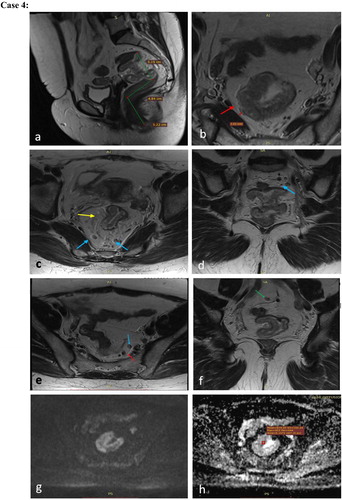
Fig. 8 (Post-neoadjuvant therapy MRI study): Post neoadjuvant CRT MRI study after 4?months revealed complete radiological response (TRG 1) yc T0-2N0. Post neoadjuvant CRT MRI with rectal distension using sonographic gel. (a), (b) and (c) Sagittal, coronal and axial high resolution T2WIs respectively showing complete response of the rectal mass lesion with no EMDI, EMVI or pathologically enlarged mesorectal nodes noted. The patient performed low anterior resection (LAR) with post-operative histopathology revealed a moderately differentiated rectal adenocarcinoma with Mandrad grade 1, 10 out of 10 nodes excised were free, Donuts free and margins free.
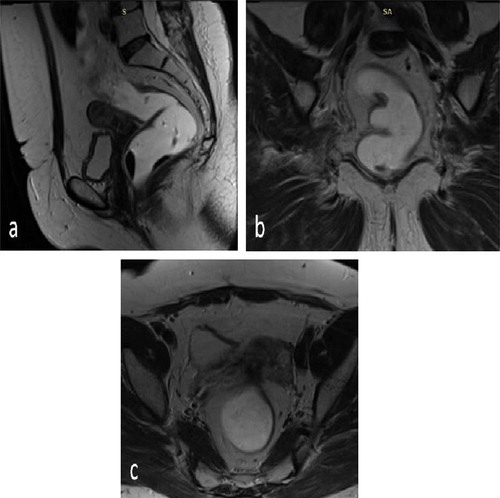
Fig. 9 (Initial MRI study): A 49?years old male patient diagnosed as rectal mass and referred from the oncology department for initial staging. Initial MRI study; (a) and (g) Sagittal high resolution T2WI, (b) through (f) Axial high resolution T2WI, (h) ADC maps showing a middle third rectal mass lesion, about 7.5?cm in maximum length, 7.8?cm from the anal verge, showing internal signal mixed with areas of cystic necrosis, involving four quadrants circumferentially; from 10 to 7o'clock. Sizable EMDI was seen with exophytic lesion about 3.2?cm in size extending from 2 to 5o'clock and invading the MRF (red arrow in b). EMVI noted at 4o'clock (yellow arrow in c). Multiple mesorectal adenopathies noted (blue arrow in d) abutting the MRF at 7o'clock (red arrow in d). Multiple extra mesorectal inferior mesenteric nodes were seen (orange arrow in e and f). The APR was noted at the upper edge of the tumor, yet not infiltrated (pink arrow in g). Restricted diffusion with ADC values about 0.8?×?10−3?mm2/s seen. The preliminary imaging based staging is c T3d N2, below APF, CRM involved.
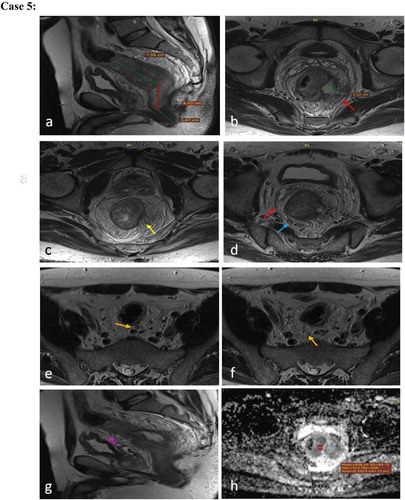
Fig. 10 (Post neoadjuvant therapy MRI): Post neoadjuvant CRT MRI study after 4?months revealed markedly responding middle rectal mass lesion …Markedly responding middle third rectal mass (TRG 2), −ve CRM, preliminary imaging based staging yc T0-2N0 Mx. Post neoadjuvant MRI study; (a) Sagittal high resolution T2WI, (b), (c) and (d) Axial high resolution T2WI, (e) and (f) DWI and ADC maps showing markedly responding middle rectal mass lesion, about 4?cm in length, 11?cm from the anorectal junction, showing predominantly hypointense SI denoting fibrotic response. The previously noted EMDI replaced by hypointense fibrotic strands (blue arrow in d), contiguous with MRF (red arrow in c). No definite diffusion restriction with ADC values 1?×?10−3?mm2/s. The patient performed total mesorectal excision (TME) with post-operative histopathology revealed a moderately differentiated rectal adenocarcinoma, 8 out of 8 nodes excised were free with fibrotic strands, Donuts free, margins free.
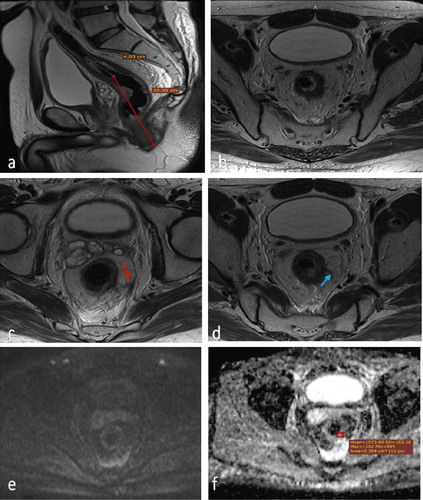
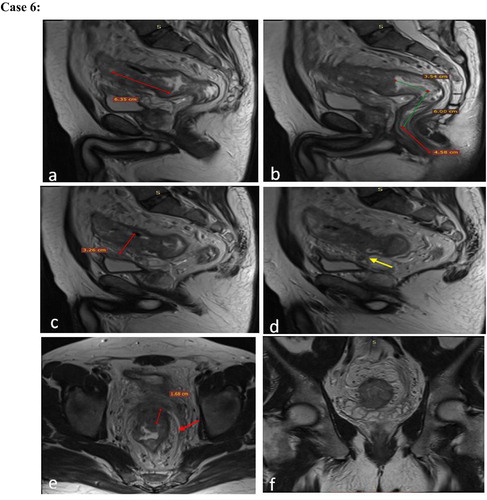
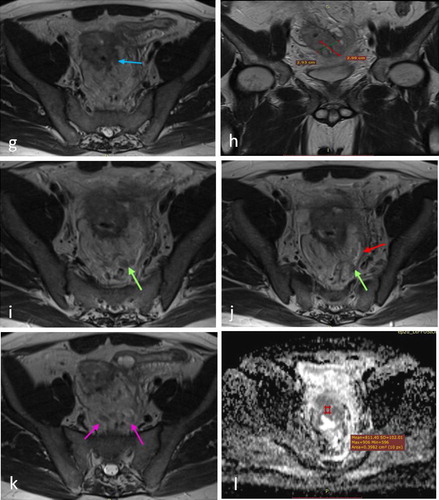
Fig. 12 (Post neoadjuvant therapy MRI): after 2?months revealed moderately responding rectosigmoid mass (TRG 3) with infiltrated APR, +CRM, preliminary imaging based staging T4a N2 Mx. MRI study with rectal distension using sonographic gel. (a) and (b) Sagittal high resolution T2WI, (c), (f) and (g) Axial high resolution T2WI, (d) and (e) Coronal high resolution T2WI, (h) ADC maps all showing moderately responding rectosigmoid mass lesion, still averaging 6?cm in length and 14?cm from the anal verge, but its maximum thickness regressed to 1.6?cm. it showed mixed intermediate and hypointense signal denoting fibrotic changes. The EMDI noted at its lower third regressed to 8?mm with multiple fibrotic strands contiguous with the MRF (red arrow in c); best depicted in c and d. Regression of the extramural component at its upper 2/3 was noted as well, averaging 2?×?1?cm in size still infiltrating the APR (best depicted in e). Regression in size of the inferior mesenteric (yellow arrow in f) and mesorectal adenopathies (green arrow in g) were seen; with distance from MRF about 2?mm. Small foci of restricted diffusion were noted with ADC values about 0.9?×?10−3?mm2/s. The patient performed trans-sphincteric resection with coloanal anastomosis, the post-operative histopathology revealed a moderately differentiated rectal adenocarcinoma, 8 out of 12 nodes excised showed malignant cells, −ve EMVI with margins free.
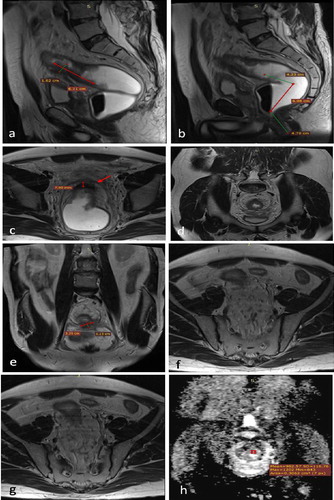
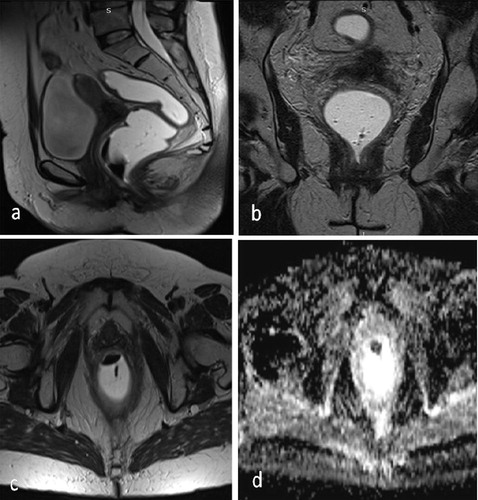
Fig. 13 (Initial MRI study): A 59?years old female patient presented with bleeding per rectum and diagnosed as rectal mass by endoscopy. Initial MRI study with rectal distension using sonographic gel. (a) Sagittal high resolution T2WI, (b) Coronal high resolution T2WI, (c) and (d) Axial high resolution T2WI, (e) and (f) DWI and ADC maps showing a lower rectal and upper anal mass lesion, about 5.3?cm in length, 3?cm in maximum thickness and about 3.3?cm from the anal verge with intermediate T2IW SI. Suspected infiltration of the puborectalis on the right side (9o'clock) was noted (yellow arrow in b). Infiltration of the rectal wall anteriorly was noted opposite to 10–11o'clock with loss of fat plane between the lesion and the posterior vaginal wall raising the possibility of local infiltration (red arrows in c). A mesorectal node showing low signal but suspicious spiculations of its contours was seen at 11o'clock (blue arrow in d). Restricted diffusion was depicted with ADC values about 0.6?×?10−3?mm2/s. The preliminary imaging based staging is c T4b N2.
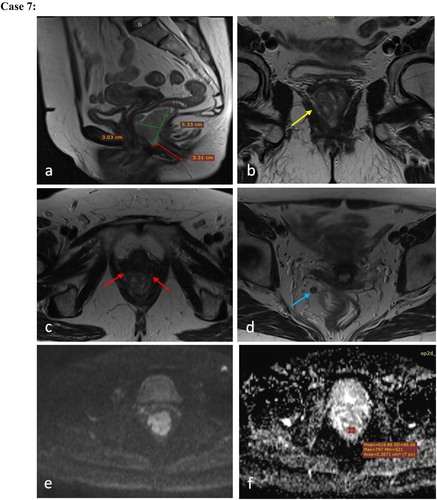
Fig. 14 (Post neoadjuvant therapy MRI): Post neoadjuvant CRT MRI study after 3 months revealed: …Complete radiologic response. No evidence of residual tumor on imaging basis: Grade 1 tumor regression grade. Imaging based staging yc T0-2N0. Post neoadjuvant MRI study with rectal distension using sonographic gel. (a), (b) and (c) Sagittal, Coronal and Axial high resolution T2WI respectively (d) ADC maps all showing total resolution of the rectal mass lesion with no suspicious adenopathies, areas of diffusion restriction or pelvic organ infiltration. The patient performed abdomino perineal resection with the post-operative histopathology revealed moderately differentiated rectal adenocarcinoma, Perineal invasion +ve, 2 out of 9 nodes excised showed malignant cells, EMVI −ve, circumferential resection margin free.