Figures & data
Figure 1. Cholecystokinin (CCK) and chromogranin A concentrations in plasma related to bodyweight in the CCKoma patient: the upper panel shows the variation in CCK concentrations from admission (december 1998) to death (august 2006). The patient was fasting at all blood samplings, even though the meal variation in plasma CCK in healthy subjects is limited (<1 to 5 pmol/l). The initial chemotherapy (I) with Octreotide-LAR and streptozotocin rapidly normalized the plasma CCK and chromogranin A (mid panel) concentrations with an effect lasting for two and a half years. In late 2001 and in 2002, the concentrations rose again. Surgical removal of the neuroendocrine tumor in the pancreas (II) was without effect on the CCK concentrations, but decreased the chromogranin A concentration in plasma slightly. The subsequent hemihepatectomy in 2003 that included the metastatic processes (III) normalized plasma CCK and chromogranin A concentrations. The lower panel shows the variations in bodyweight: after an initial decrease the weight increased rapidly during 1999 after onset of chemotherapy. A new period of weight loss accompanied the recurrence of the diarrheas and the gradual increase in plasma CCK and chromogranin A concentrations. Finally, after hemihepatectomy with normalization of CCK in plasma and absence of diarrheas, the weight increased again. Recurrence of liver metastases in 2004-5 resulted again in increased plasma chromogranin A concentrations, but had no effect on CCK production. From ref. Citation17 with permission.
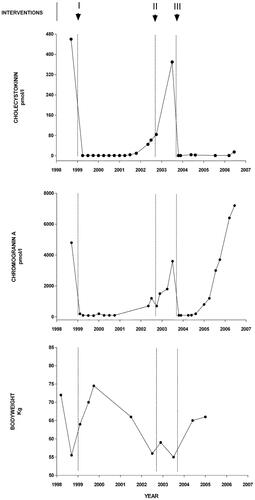
Figure 2. Bioactive CCK and proCCK forms in a plasma sample from the CCKoma patient: by size-chromatography on a calibrated sephadex G50 superfine column, four peptides eluted like CCK-83, -58, -33, and -8 using a specific radioimmunoassay for bioactive, amidated CCK [Citation29]. the assay measures the CCK-forms with equimolar potency without cross-reactivity with homologous gastrin peptides (upper panel). A radioimmunoassay for human proCCK identified in the same plasma sample intact proCCK and three N-terminally truncated forms of proCCK (lower panel). Note the 10-fold higher concentrations of proCCK fragment in the lower panel. From ref. [Citation17] with permission.
![Figure 2. Bioactive CCK and proCCK forms in a plasma sample from the CCKoma patient: by size-chromatography on a calibrated sephadex G50 superfine column, four peptides eluted like CCK-83, -58, -33, and -8 using a specific radioimmunoassay for bioactive, amidated CCK [Citation29]. the assay measures the CCK-forms with equimolar potency without cross-reactivity with homologous gastrin peptides (upper panel). A radioimmunoassay for human proCCK identified in the same plasma sample intact proCCK and three N-terminally truncated forms of proCCK (lower panel). Note the 10-fold higher concentrations of proCCK fragment in the lower panel. From ref. [Citation17] with permission.](/cms/asset/5c053ecc-3069-4a45-8289-09284624ab6c/igas_a_2308532_f0002_b.jpg)
Figure 3. Scheme of structurally identified α-amidated products of proCCK. The cleavage sites at basic amino acid residues (R (arginine) and K (lysine)) are indicated on proCCK. s and ns mean ‘sulfated’ and ‘nonsulfated’ respectively.
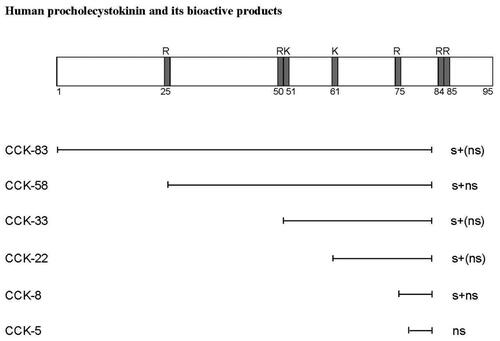
Figure 4. The primary structure of the C-terminal heptapeptide amide sequence that constitutes the specific receptor epitope of bioactive CCK peptides. The corresponding gastrin sequence is aligned below. Note the difference in the position of the tyrosyl residues between CCK and gastrin peptides.
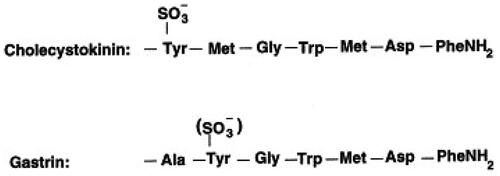
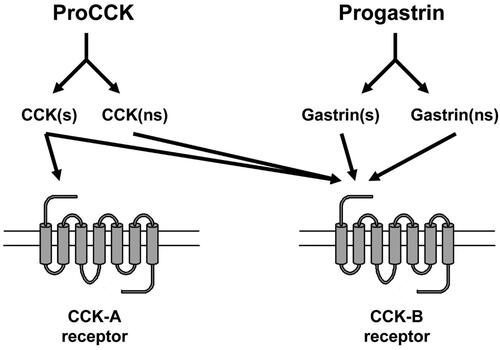
Figure 5. The homologous hormone precursors proCCK and progastrin are both processed to sulfated (s) and nonsulfated (ns) bioactive peptides. Only sulfated CCK peptides are, however, bound with high affinity to the CCK-A receptor, whereas the CCK-B receptor binds all the α-amidated peptide products of both proCCK and progastrin.