
Figures & data
Table 1. Baseline patient and breast cancer characteristics at the time of first diagnosis.
Table 2. Patient and tumour characteristics at the onset of HT combined with re-RT.
Table 3. Evaluation of tumour response upon termination of combined HT + re-RT treatment.
Table 4. Clinical outcome of combined HT + re-RT treatment.
Figure 1. Relative spectral irradiance of a halogen lamp (correlated colour temperature CCT =3000 K) as a function of wavelength, before (curve 1) and after passing a water-filter and a cut-off filter (BTE, Elsoff, Germany) (curve 2). Measurements by using a double monochromator spectroradiometer (Spectro 320 D, Instrument Systems, Munich, Germany) in the spectral range 0.4–1.7 μm) and calculation of data according to Planck’s law of radiation in the spectral range 1.7–4.5 μm. VIS: visible light spectrum
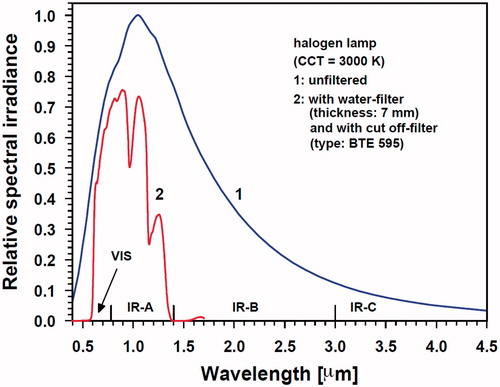
Figure 2. Measurement of surface temperature with contact electrodes (type PT100). Placement of sensor (upper left panel), fixation (upper right panel) and absolute temperature reading (lower left panel). Corresponding thermography (lower right panel).
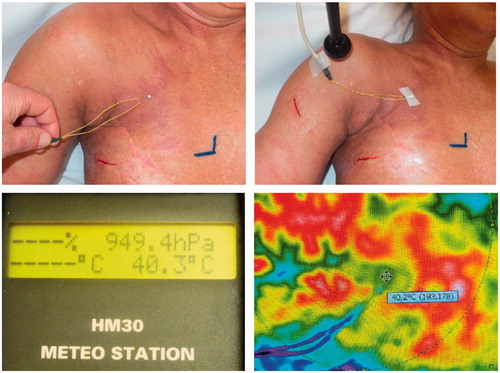
Figure 3. Thermographic control of wIRA-hyperthermia in a patient with inflammatory breast cancer recurrence. Before start of heating: (a) visible inflammatory disease, (b) scar of the former tumourectomy, (c) field-mark for RT, (d) subcutaneous venous drainage, and (e) sebaceous retention cyst. Immediately after start of hyperthermia and within 19 s the venous drainage increases and transports heat away (cooling effect). After a few minutes this effect is clearly visible, then a breakdown of blood flow can be seen (after 2.5 min). These latter effects disappear after 3 min. Inflammatory recurrence and/or scarred tissue are heated up to 43 °C after 2.5 min and stay at this higher temperature level during the whole treatment period (see the bottom line at 20 and 45 min).
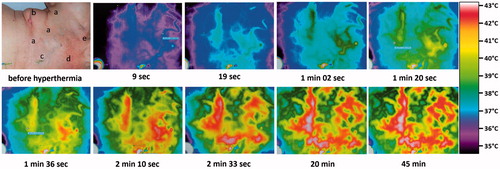
Figure 4. Inflammatory recurrent breast cancer in a 51-years old patient. Former conservative therapy for triple negative breast cancer consisting in tumourectomy, sentinel lymphadenectomy, adjuvant chemotherapy and radiotherapy with 50 Gy whole breast and boost up to 60 Gy. First recurrence treated with salvage surgery, chemotherapy followed by breast reconstruction. Top: Situation before start of re-RT and wIRA-HT (21.6.2011, patient in treatment position). Several biopsies on both breasts confirmed the inflammatory recurrence. Middle: First thermographically controlled wIRA-HT of both chest wall regions. Bottom: 4 years after completion of hypofractionated re-RT with 5 × 4 Gy and wIRA-HT (NED, 21.9.2015, patient in sitting position). Teleangiectasias are evident especially in the décolleté and the former irradiated region
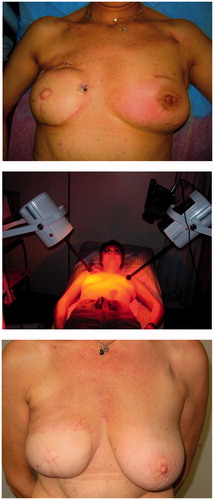
Figure 5. Mean temperature profiles within tissues during wIRA-exposure under steady state conditions. Curve 1: Calculated by averaging measured data in normal tissues (Hellige in Ref. [Citation11], open squares), tumour tissues (Seegenschmiedt et al. [Citation31], circles) and in recurrent breast cancers (Notter et al., current report, red triangles). Curve 2: temperature profile in untreated skin and subcutis, i.e., no wIRA exposure (Hellige in Ref. [Citation11], filled squares).
![Figure 5. Mean temperature profiles within tissues during wIRA-exposure under steady state conditions. Curve 1: Calculated by averaging measured data in normal tissues (Hellige in Ref. [Citation11], open squares), tumour tissues (Seegenschmiedt et al. [Citation31], circles) and in recurrent breast cancers (Notter et al., current report, red triangles). Curve 2: temperature profile in untreated skin and subcutis, i.e., no wIRA exposure (Hellige in Ref. [Citation11], filled squares).](/cms/asset/c86adc7d-48f8-475e-9ee3-b32473c80553/ihyt_a_1235731_f0005_c.jpg)
Figure 6. Top left: Overall survival of 73 patients with locally recurrent breast cancer treated with re-irradiation and wIRA-hyperthermia. Top right: Overall survival of 64 patients (macroscopic disease) with locally recurrent breast cancer treated with re-irradiation and wIRA-hyperthermia. Middle left: Influence of local control on survival after CR. 32 patients had local control throughout life time (upper curve), 16 patients presented with re-recurrences (lower curve). Difference is statistically significant (log rank test p = .03). Middle right: Influence of lymphangiosis carcinomatosa on survival. Forty-six patients had lymphangiosis carcinomatosa (lower curve), 18 patients presented with macroscopic disease without lymphangiosis (upper curve). Difference is statistically significant (log rank test p < .001). Bottom left: Local progression-free survival until re-recurrence after CR (n = 48). Bottom right: Local progression-free survival until re-recurrence or patient death after CR (n = 48).
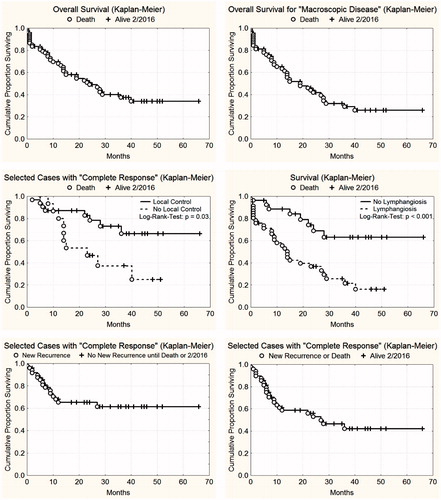
Table 5. Side effects upon HT + re-RT of recurrent breast cancers.
Table 6. Combination of RT and HT in pre-irradiated, recurrent breast cancer: Review of available data.