Figures & data
Table I. Diagnostic Guidelines for HLH.
Table II. Spectrum of diseases characterized by hemophagocytosis.
Figure 1. Graphical representation of the genes involved in cytotoxic granule formation, secretion, and target cell death. The first step in cellular cytotoxicity is the development of functional granules containing effector molecules(e.g. perforin, granzymes) and regulatory molecules (e.g. DPP1, serglycin, and calreticulin). Once an effector cell makes a functional secretory synapse through the interactions of adhesion molecules (e.g. LFA‐1/ICAM‐1), signal transduction events (e.g. SAP/SLAM) are initiated resulting in cell polarization by polymerization of actin/microtubules towards the secretory synapse (e.g. WASp). The preformed cytotoxic granules migrate to the secretory synapse using myosin proteins (e.g. Myo5a) and are released from the actin filaments (e.g. Rab27a) at the plasma membrane. Fusion of the granules with the plasma membrane occurs (e.g. Lyst, Munc13‐4) and effector molecules are released into the synapse. Perforin then polymerizes into pore‐forming structures in the target cell membrane that ultimately allow for the entry of granzymes into the cytoplasm of the target cells through a yet undefined mechanism. The granzymes subsequently induce apoptosis of the target cell through the cleavage/activation of multiple pro‐apoptotic target molecules in the cytoplasm, mitochondria, and nucleus. LFA‐1 = lymphocyte function associated antigen 1; ICAM‐1 = intercellular adhesion molecule 1; Lyst = lysosomal trafficking regulator gene.
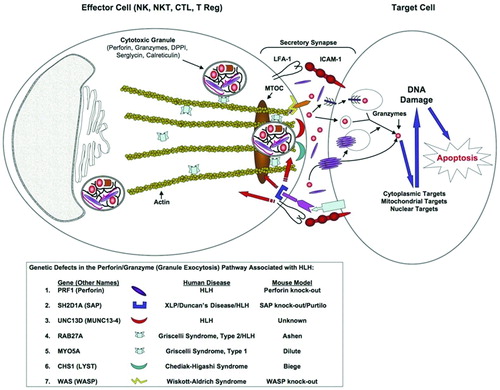
Figure 2. Hemophagocytic lymphohistiocytosis(HLH) results from a failure of immune cell contraction due to defects in cytotoxicity. Early in the immune response, CD4 and CD8 lymphocytes are activated by antigen presenting cells and expand to be able to clear infectious pathogens. Once an effective immune response is established and the pathogens are eradicated, the expanded immune repertoire must contract to keep the relative number of lymphocytes constant. This contraction phase is dependent on cytotoxicity of lymphocytes. This may be mediated by CD8 lymphocytes, natural killer cells, or possibly by the cytotoxic T regulatory cells. Without this contraction phase, the immune response proceeds unchecked as is seen in hemophagocytic lymphohistiocytosis, resulting in the demise of the affected patients without treatment. APC: antigen presenting cell.
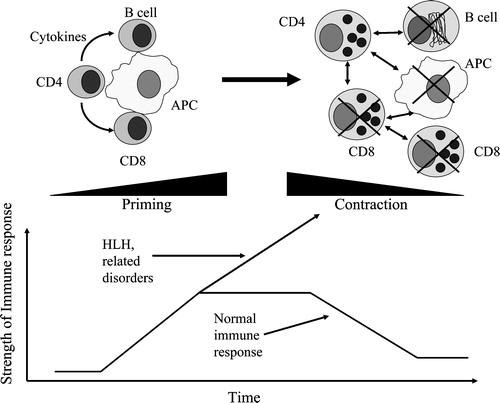
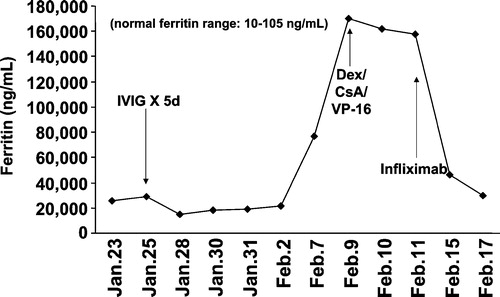
Figure 3. Effective treatment of a refractory hemophagocytic lymphohistiocytosis patient with Infliximab(anti‐TNF‐α). Briefly, the 16‐year‐old male subject had EBV‐associated hemophagocytic lymphohistiocytosis (HLH) that was refractory to IVIG, steroids, and VP‐16, leading to pulmonary failure and mechanical ventilation. Upon institution of Infliximab therapy his clinical status improved significantly within 24–48 hours, represented by a marked decrease in his serum ferritin levels and improvement of all clinical parameters including removal from mechanical ventilation.