
Figures & data
Figure 1: Room setting, with laparoscopy stack placed at the patient’s head, with patient’s thighs abducted and internally rotated to access femoral triangle.

Figure 2: (A) 10 mm vision port placed 2 mm caudal to the apex of the femoral triangle with telescope inserted. (B) Second trocar (5 mm) inserted under vision 5 cm medial to the vision port. (C) All THREE ports inserted and working space developed further cranially.

Figure 3: Undermining the skin flap below the Scarpa fascia and cranial extension of the working space.
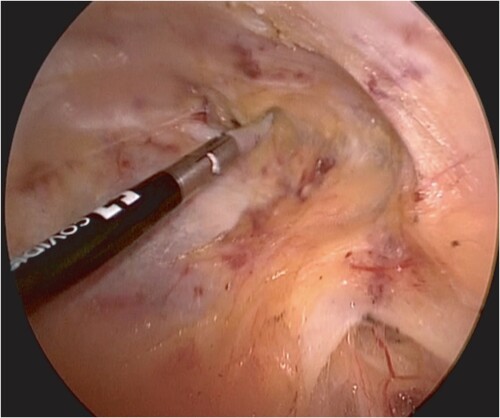
Figure 4: Removal of lymph node basin.
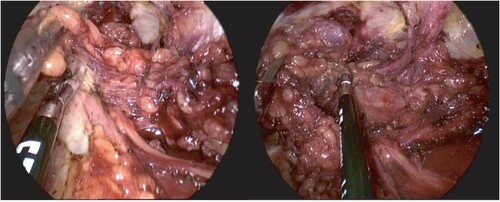
Figure 5: Lymph node basin removed with identification and sparing of the great saphenous vein.
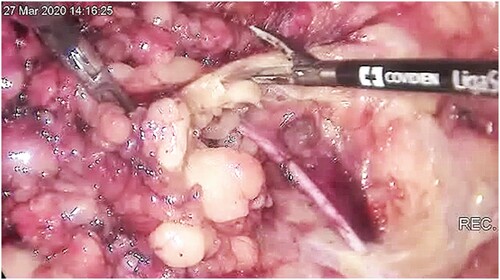
Figure 6: Closure and suction drain inserted.

Table 1: Patients’ background characteristics
Table 2: Perioperative and pathological characteristics
Table 3: Lymph node harvest for each groin by L-MILND
Table 4: Postoperative complications