
Figures & data
Table 1. Distribution of the studied groups regarding demographic data.
Graph 1. Distribution of the studied patients regarding the functional outcome.
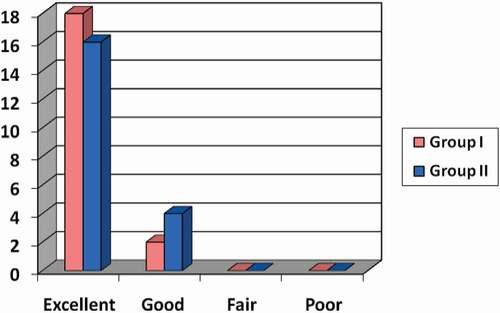
Table 2. Relations between MSTS parameters at the end of the follow-up period between both groups.
Figure 1. A 43-year-old male patient with Rt GCT distal femur (group I). (a and b) AP and lateral X-ray of Rt knee showing osteolytic lesion affecting medial femoral condyle. (c and d) Coronal & axial T1 weight MRI showing hypointense lesion with cortical thinning without soft tissue extension. (e−g) Intraoperative photos showing the reconstruction of the medial femoral condyle after extended curettage with subchondral iliac bone graft followed by gel foam and cement. (h and i) AP and lateral x-ray of Rt knee immediately postoperative. (j and k) AP and lateral X-ray of Rt knee at the end of follow-up period showing full incorporation of bone graft and no evidence of recurrence.
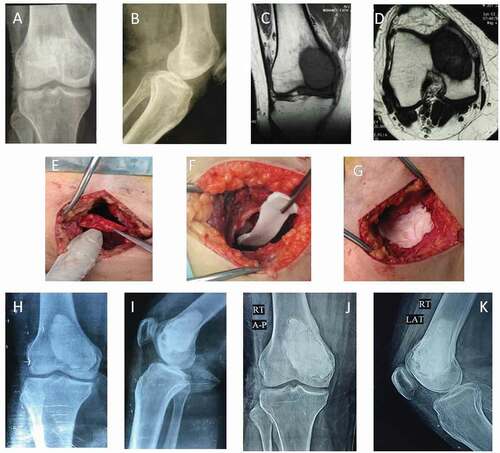
Figure 2. A 24-year-old female patient with Lt GCT distal femur (group II) with pathological fracture. (a and b) AP and lateral X-ray of Rt knee showing osteolytic lesion affecting medial femoral condyle with pathological fracture. (c and d) Coronal and axial CT delineating the fracture pattern and cortical thinning of the condyle. (e and f) Coronal and axial T2-weighted MRI showing isointense lesion with intralesional fluid signals of hemorrhage without soft tissue extension. (g and h) Intraoperative photos showing extended curettage. (i-k) Intraoperative photos showing fixation of fracture with 2 k-wires with subchondral iliac bone graft and cement. (l and m) AP and lateral x-ray of Rt knee immediately postoperative. (n and o) AP and lateral X-ray of Rt knee at the end of follow-up period showing full incorporation of bone graft and no evidence of recurrence. (p and q) AP and lateral x-ray of Rt knee; the prominent k wire was painful, which requires its removal.
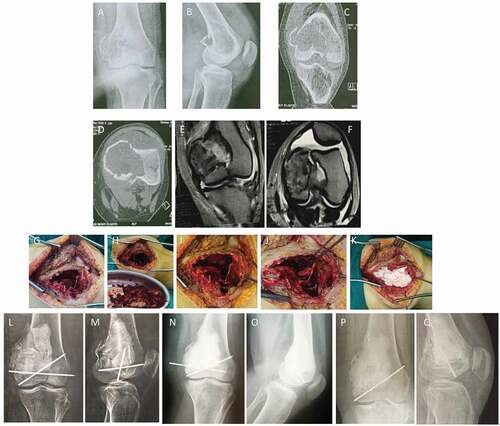
Table 3. Distribution of the studied patients regarding Kellgren-Lawrence grading for osteoarthritis.