Figures & data
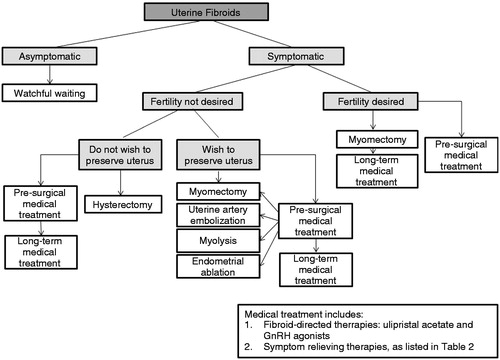
Figure 1. Factors involved in UF formation and growth. Adapted from Islam et al. 2013Citation14.
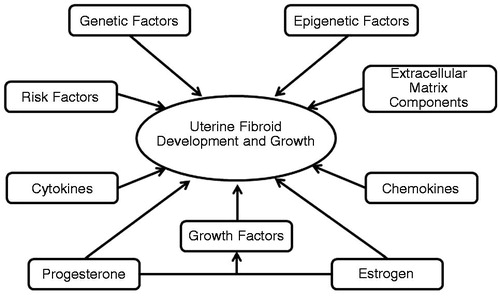
Figure 2. Uterine fibroid subclassification within the FIGO abnormal uterine bleeding classification system. Intracavitary lesions are attached to the endometrium by a narrow stalk and are classified as Type 0, whereas Types 1 and 2 require a portion of the lesion to be intramural – with Type 1 having less than 50% involvement and Type 2 at least 50%. Type 3 lesions are totally extracavitary but abut the endometrium. Type 4 lesions are intramural UFs that are entirely within the myometrium, with no extension to the endometrial surface or to the serosa. Subserosal (Types 5–7) UFs represent the mirror image of the submucosal UFs – with Type 5 being at least 50% intramural, Type 6 less than 50% intramural, and Type 7 attached to the serosa by a stalk. An additional category, Type 8, is reserved for UFs that do not relate to the myometrium at all, and would include cervical lesions, those that exist in the round or broad ligaments without direct attachment to the uterus, and other so-called ‘parasitic’ lesions. Hybrid UFs are transmural and are classified by their relationship to both the endometrial and serosal surfaces. Two numbers are separated by a hyphen (e.g., 2–5); the first refers to the relationship with the endometrium, while the second refers to the relationship with the serosa. Reprinted with permission from Munro et al., 2011Citation31.
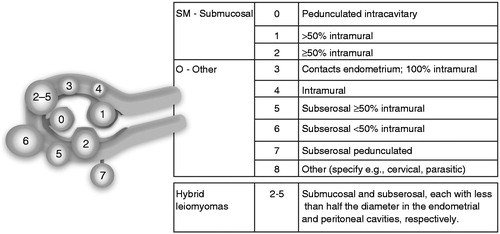
Table 1. Factors associated with the risk of uterine fibroids.
Table 2. Summary of treatment options for uterine fibroids.
Figure 3. Uterine fibroid treatment algorithm. Please refer to for advantages and disadvantages of the different therapeutic approaches.