Figures & data
Table 1. WHO-recommended treatment strategy for schistosomiasis.
Table 2. WHO vision, goals and objective for control of schistosomiasis.
Table 3. List of key needs and resources for deworming at the school site.
Table 4. Summary of characteristics of trials selected after systematic review evaluating single dose praziquantel (40 mg/kg) treating urogenital and intestinal schistosomiasis in children.

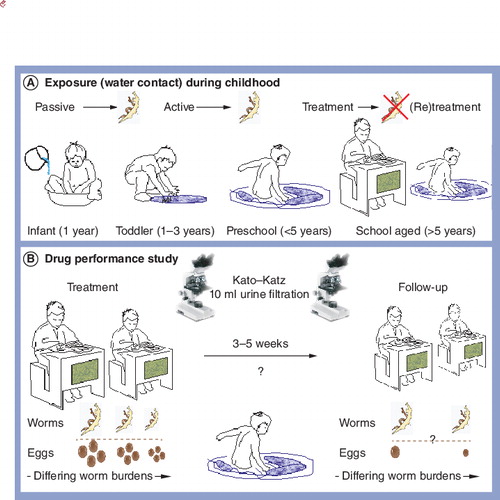
![Figure 4. Generic information, education and communication materials produced by WHO for implementing preventive chemotherapy within schools.(A) Front cover of teacher training booklet for deworming school children. (B) On-site tools needed for administration of deworming tablets to children: potable water, drinking cups and praziquantel height pole is needed alongside treatment registers for recording treatments and noting any noncompliance or side effects.Figure taken from Citation[14].](/cms/asset/35bb7f72-1968-4b2e-8c50-d1018b5eb56a/ierz_a_811931_f0004_b.jpg)