Figures & data
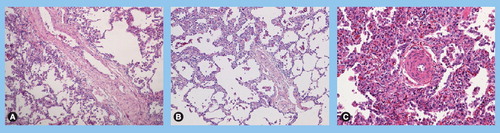
(A) Vascular remodeling in a patient with pulmonary veno-occlusive disease (PVOD): septal vein displaying loose fibrosis with cushion-like narrowing of the native lumen. (B) Vascular remodeling in a patient with PVOD: preseptal venules with occlusive intimal fibrosis; note the partial thickening of alveolar septa due to focal multiplication of alveolar capillaries. (C) Vascular remodeling in a patient with PVOD: associated precapillary remodeling in the same patient with typical hyperplasia of small arterioles; note numerous intra-alveolar macrophages and capillary filling/multiplication as indirect signs of congestion due to post-capillary obstruction. (A–C) Hematoxylin-eosin stained, magnification ×100.
This diagram explains why pulmonary capillary wedge pressure (PCWP) is usually normal in pulmonary veno-occlusive disease (PVOD). PVOD mostly affects small pulmonary veins, leading to an elevation of pressure in this region (Pv), as well as to an elevation in true pulmonary capillary pressure (Pc) and precapillary pulmonary arterial pressure (Pa). Larger pulmonary veins are usually not affected by PVOD, and it is in fact the pressure here that is reflected by PCWP: the static column of blood (hatched) occluded by pulmonary arterial catheter wedging or balloon inflation of a pulmonary arterial branch (balloon 1) reflects the pressure in a vein of similar diameter (balloon 2), usually of a larger size than those vessels affected by PVOD. Therefore, this measurement technique does not reflect the important elevation of pressure in the smaller diameter vessels associated with PVOD.
Reprinted with permission from Citation[5].
![Figure 2. Measurement of pulmonary capillary wedge pressure in pulmonary veno-occlusive diseaseThis diagram explains why pulmonary capillary wedge pressure (PCWP) is usually normal in pulmonary veno-occlusive disease (PVOD). PVOD mostly affects small pulmonary veins, leading to an elevation of pressure in this region (Pv), as well as to an elevation in true pulmonary capillary pressure (Pc) and precapillary pulmonary arterial pressure (Pa). Larger pulmonary veins are usually not affected by PVOD, and it is in fact the pressure here that is reflected by PCWP: the static column of blood (hatched) occluded by pulmonary arterial catheter wedging or balloon inflation of a pulmonary arterial branch (balloon 1) reflects the pressure in a vein of similar diameter (balloon 2), usually of a larger size than those vessels affected by PVOD. Therefore, this measurement technique does not reflect the important elevation of pressure in the smaller diameter vessels associated with PVOD.Reprinted with permission from Citation[5].](/cms/asset/a719f678-5ad3-4795-9cbd-f7451610e1c6/ierx_a_11219173_f0002_b.jpg)
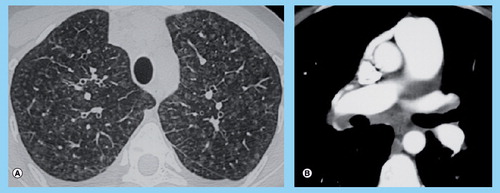
(A) High-resolution computed tomography of the chest showing marked ground-glass opacities with centrilobular pattern, ground-glass opacities with poorly defined nodular opacities, septal lines. (B) High-resolution computed tomography of the chest showing mediastinal lymph node enlargement.