
Figures & data
Figure 1 Acute cutaneous lupus erythematosus (ACLE) characterized by violaceous to erythematous patches and thin plaques involving the malar cheeks. Importantly, this pathognomonic “butterfly rash” of lupus strikingly spares the nasolabial folds helping to distinguish ACLE from disease mimics.

Figure 2 Annular subacute cutaneous lupus erythematosus (SCLE) characterized by polycyclic violaceous annular plaques with trailing scale in photo distributed anatomic sites (eg, upper chest).

Figure 3 Discoid lupus erythematosus (DLE) has a predilection for the conchal bowls, face, and scalp, and presents with erythematous to violaceous scarring plaques with overlying adherent scale and follicular plugging.

Table 1 Systemic Lupus International Collaborating Clinics (SLICC) Criteria*
Figure 4 Gottron’s papule appearance varies across skin tones presenting as pink to violaceous to hyperpigmented macules and papules over dorsal hands with predominance over metacarpophalangeal joints.
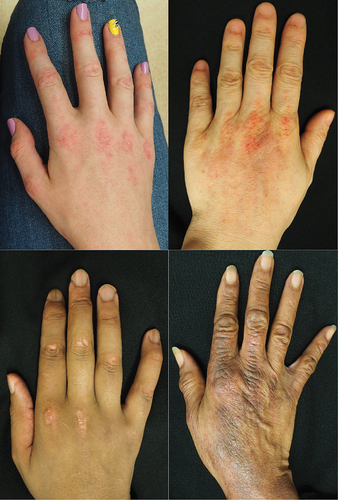
Figure 5 Nailfold capillary changes of dermatomyositis involve dilated capillary loops alternating with avascular areas and cuticular hemorrhage.
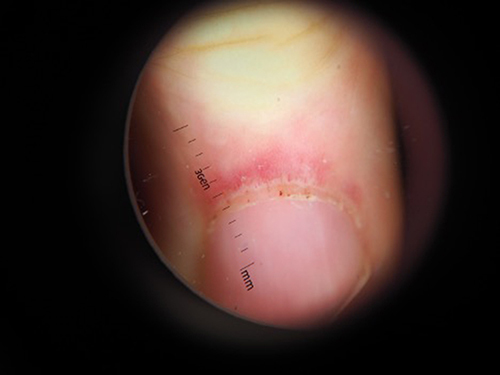
Table 2 Common Myositis Specific Antibodies in Dermatomyositis
Figure 6 Cutaneous fibrosis starting at the distal fingers, as demonstrated by decreased skin mobility between the distal interphalangeal and proximal interphalangeal joints (A) is one of the hallmark features of systemic sclerosis. Over time, fibrosis extends proximally leading to difficulties forming a fist (B) and a positive “prayer sign” (C).
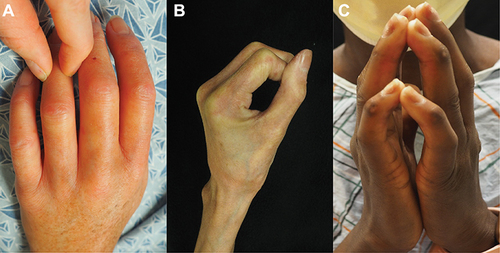
Figure 7 Salt-and-pepper dyspigmentation can be the presenting finding in patients with systemic sclerosis and a leading cause of body image dissatisfaction in patients with skin of color.

Table 3 Summary of French Recommendations for the Workup and Management of Systemic Sclerosis (SSc)Citation135
Figure 8 Plaque morphea is a subtype of morphea characterized by <3 plaques and <3 centimeters in size.

Figure 9 En coup de sabre is a subtype of linear morphea presenting as a hyper to hypopigmented indurated plaque extending linearly down the paramedian or temporal forehead.

Figure 10 The groove sign of eosinophilic fasciitis is characterized by linear indentations of skin along the superficial veins of the forearm.

Figure 11 Preservation of mobility of the skin between the distal interphalangeal and proximal interphalangeal joints can help distinguish eosinophilic fasciitis from systemic sclerosis.

Figure 12 Fibrosis along the fascial plane in eosinophilic fasciitis can produce a puckering of skin of the proximal upper and lower extremities leading to a “pseudo-cellulite” type appearance.
