Figures & data
Figure 1 Rheumatoid arthritis and ulcerative colitis patient attrition in samples derived from the US MarketScan® Databases. A total of 111,137 patients with RA and 47,611 patients with UC had the two diagnosis codes required for this study. Application of other eligibility criteria reduced this to 73,364 patients with RA, to give three 33% samples of 24,373 patients with RA each, and 29,072 patients with UC, to give three 33% samples of 9665 patients with UC each. Controls were exact matched 3:1 to cases according to age, sex, region, and insurance type (Medicare-supplemental or commercial). Those eligible patients who could not be exact matched to controls (245 patients with RA and 77 patients with UC) were excluded from the study.
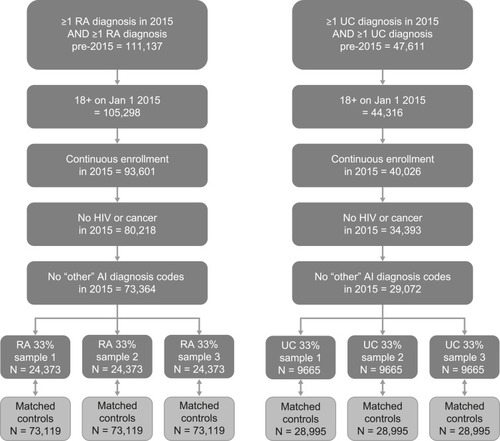
Table 1 Patient Demographics And Baseline Characteristics In The Three (A) Rheumatoid Arthritis Samples And (B) Ulcerative Colitis Samples And Their Matched Controls
Figure 2 Percentage of total healthcare cost attributed to disease (ie, percentage disease-related cost) for patients with rheumatoid arthritis or ulcerative colitis according to analysis method. aMethod 4 not executed in the UC sample. The different methods used to assess healthcare cost attributed to disease for patients with RA and UC were as follows: Method 1, claim-wide cost attribution based on claim-listed diagnosis codes and a predetermined disease-related medication list (pharmacy claims only); Method 2, line-item cost attribution based on procedures/medications more likely to occur in cases than in matched controls at two likelihood ratio cutoffs (1.5× and 3.5×); Method 3, disease-related cost calculated as the difference in total average cost between cases and their matched controls; Method 4, line-item cost attribution based on clinician manual determination of procedures/medications related to the disease; this method served as an internal standard method and was applied only in patients with RA.
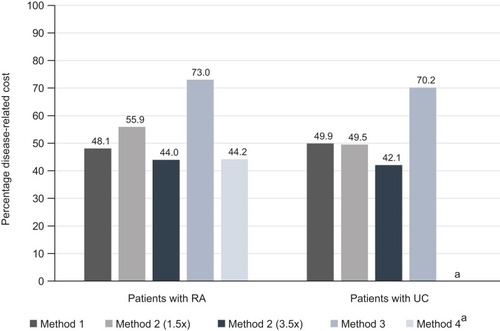
Figure 3 Total healthcare cost by attribution method and cost component per patient for patients with (A) rheumatoid arthritis and (B) ulcerative colitis. The different methods used to assess healthcare cost attributed to disease for patients with RA and UC were as follows: Method 1, claim-wide cost attribution based on claim-listed diagnosis codes and a predetermined disease-related medication list (pharmacy claims only); Method 2, line-item cost attribution based on procedures/medications more likely to occur in cases than in matched controls at two likelihood ratio cutoffs (1.5× and 3.5×); Method 3, disease-related cost calculated as the difference in total average cost between cases and their matched controls; Method 4, line-item cost attribution based on clinician manual determination of procedures/medications related to the disease; this method served as an internal standard method and was applied only in patients with RA.
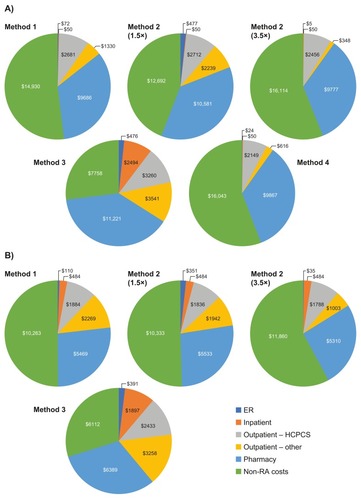
Figure 4 Disease-related healthcare resource utilization by attribution method and component for patients with (A) rheumatoid arthritis and (B) ulcerative colitis. The different methods used to assess healthcare resource utilization attributed to disease for patients with RA and UC were as follows: Method 1, claim-wide HCRU attribution based on claim-listed diagnosis codes and a predetermined disease-related medication list (pharmacy claims only); Method 2, line-item HCRU attribution based on procedures/medications more likely to occur in disease cases than in matched controls at two likelihood ratio cutoffs (1.5× and 3.5×); Method 3, disease-related HCRU calculated as the difference in total average HCRU between disease cases and their matched controls; Method 4, line-item HCRU attribution based on clinician manual determination of procedures/medications related to the disease; this method served as an internal standard method and was applied only in patients with RA. All data shown as mean values, with error bars representing standard deviation of the mean.
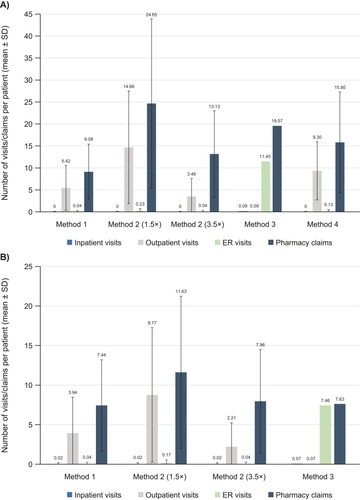
Figure 5 Disease-related cost per patient by attribution method across subgroups of patients with (A) rheumatoid arthritis, and (B) ulcerative colitis. The different methods used to assess healthcare cost attributed to disease for patients with RA and UC were as follows: Method 1, claim-wide cost attribution based on claim-listed diagnosis codes and a predetermined disease-related medication list (pharmacy claims only); Method 2, line-item cost attribution based on procedures/medications more likely to occur in disease cases than in matched controls at two likelihood ratio cutoffs (1.5× and 3.5×); Method 3, disease-related cost calculated as the difference in total average cost between disease cases and their matched controls; Method 4, line-item cost attribution based on clinician manual determination of procedures/medications related to the disease; this method served as an internal standard method and was applied only in patients with RA. Patient subgroups were those who received biologic therapy or had advanced disease versus those without biologic therapy or advanced disease, and those with an ER visit versus those who did not visit the ER.
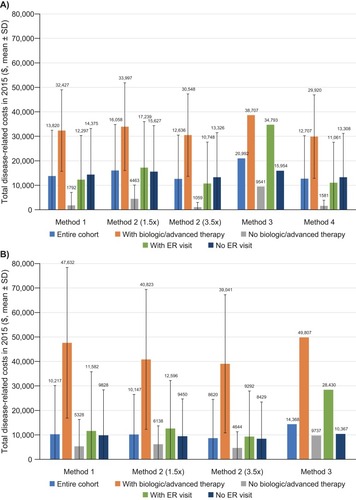
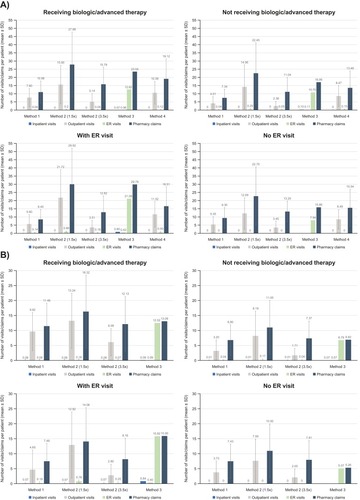
Figure 6 Disease-related healthcare resource utilization by attribution method and component across subgroups of patients with (A) rheumatoid arthritis and (B) ulcerative colitis. The different methods used to assess healthcare resource utilization attributed to disease for patients with RA and UC were as follows: Method 1, claim-wide HCRU attribution based on claim-listed diagnosis codes and a predetermined disease-related medication list (pharmacy claims only); Method 2, line-item HCRU attribution based on procedures/medications more likely to occur in disease cases than in matched controls at two likelihood ratio cutoffs (1.5× and 3.5×); Method 3, disease-related HCRU calculated as the difference in total average HCRU between disease cases and their matched controls; Method 4, line-item HCRU attribution based on clinician manual determination of procedures/medications related to the disease; this method served as an internal standard method and was applied only in patients with RA. Patient subgroups were those who received biologic therapy or had advanced disease versus those without biologic therapy or advanced disease, and those with an ER visit versus those who did not visit the ER. Values are shown as mean ± standard deviation.