
Figures & data
Figure 1 Structure of the chelating drugs.
Notes: The chemical and physicochemical properties of chelating drugs influence their clinical activity, including their mode of action, organ targeting, efficacy, and toxicity. Deferiprone and deferoxamine are hydrophilic chelators that increase iron excretion and decrease iron absorption. Maltol, deferasirox, and 8-hydroxyquinoline are lipophilic chelators that form lipophilic metal complexes, and can cause an increase in iron and other metal absorption. Orally absorbed, nonmetal-bound deferasirox mobilizes excess iron, mainly from the liver, and causes an increase in iron excretion. The pharmacological effects of different drugs, eg, hydroxycarbamide (hydroxyurea) are affected by iron binding.
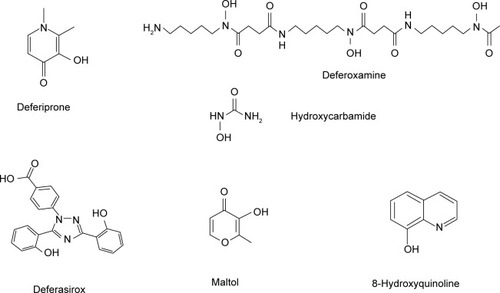
Table 1 Examples of thalassemia intermedia and other conditions where iron overload can be caused from the increased gastrointestinal absorption of ironTable Footnote*
Figure 2 Iron-absorption and iron-overload mechanisms in non-transfusion-dependent thalassemias: the role of chelators and chelating drugs.
Notes: Mechanism of iron absorption at the enterocyte using regulatory pathways of iron metabolism involving DMT1, hepcidin, ferroportin, and transferrin. Increased gastrointestinal iron absorption and iron overload is observed in non-transfusion-dependent thalassemias, due to ineffective erythropoiesis in the bone marrow (A). The level of increased iron absorption depends on the form and quantity of iron present in the diet and other factors, such as the presence of natural or synthetic iron chelators in the gastrointestinal tract. Iron-chelating drugs and other chelators have variable pharmacological effects on iron absorption, with lipophilic chelators causing an increase in iron absorption and hydrophilic chelators a decrease in iron absorption. Excess iron absorption causes iron overload and damage in the liver, the heart, and other organs. The liver is the main organ of excess iron deposition, whereas the heart is the most susceptible organ of iron toxicity, as a result of iron overload from increased iron absorption. Iron overload in both the liver (B) and the heart (C) in non-transfusion-dependent thalassemia are the main target sites of chelation therapy.
Abbreviations: DMT1, divalent metal transporter 1; EDTA, ethylenediaminetetraacetic acid; DTPA, diethylenetriaminepentaacetic acid.
Abbreviations: DMT1, divalent metal transporter 1; EDTA, ethylenediaminetetraacetic acid; DTPA, diethylenetriaminepentaacetic acid.
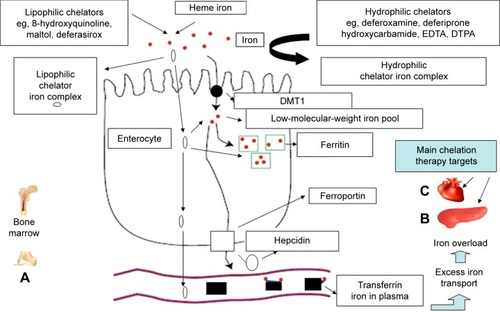
Table 2 Examples of nonregulatory factors affecting iron absorptionTable Footnote*
Table 3 Mode of action and property differences of the chelating drugs deferoxamine, deferiprone, and deferasirox and other chelatorsTable Footnote*