Figures & data
Table 1 Comparison of the oxygenation in organs and respective tumors
Figure 1 Regulation of HIF in normoxic and hypoxic conditions.
Notes: HIF-α, a transcription factor, can be regulated by both hypoxic and non-hypoxic factors. In normoxia, HIF-α subunits are hydroxylated by oxygen sensors, including PHD and FIH-1 enzymes, causing polyubiquitination and proteasomal degradation of hydroxylated HIF-α subunits (red arrows). PHD and FIH-1’s activity is oxygen-dependent (red arrows); in hypoxia (blue arrows) these enzymes lose their activity due to decreased oxygenation, resulting in HIF-α protein stabilization, accumulation, and translocation into the nucleus resulting in gene transcription and biological consequences (black arrows). HIF is also modulated in a hypoxia-independent manner in response to nitric oxide (NO), reactive oxygen species (ROS), cytokines, lipopolysaccharides, and growth factors through receptor tyrosine kinases (RTK), G protein-coupled receptors (GPCRs), toll-like receptors (TLR) and alarmins receptors. The non-hypoxic HIF regulation is mediated by a number of different signaling pathways including NFκB, PI3K/AKT/mTOR, and MAPK/ERK (green arrows). These pathways, as well as ROS production, are additionally regulated by hypoxia, which results in multiple levels of HIF-α stimulation, both hypoxic and normoxic. As a result, HIF accumulation and activation alters blood vessel formation, apoptosis, metastasis, and metabolism via a number of genes including VEGF, SDF-1, Ang-2, MMPs, BNIP-3, p53, epithelial-to-mesenchymal transition (EMT), E-cad, CXCR4, LOX, CAIX, GLUT-1, and GSK (black arrows).
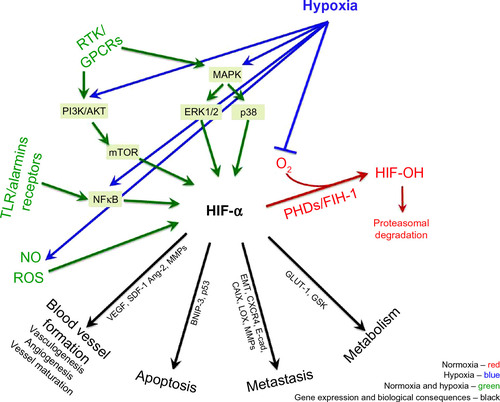
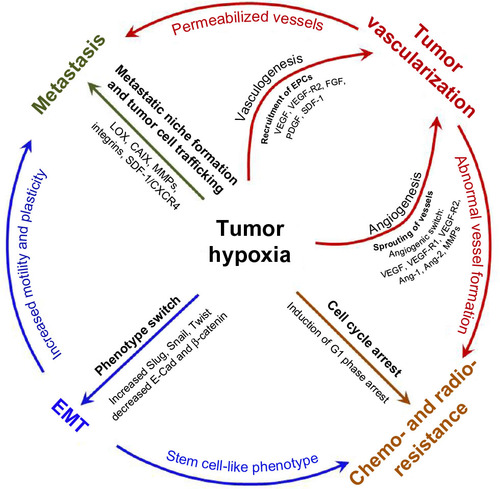
Figure 2 Hypoxia as a driving force of tumor progression and metastasis.
Notes: Hypoxia stimulates tumor i) vasculogenesis through endothelial progenitor cells’ mobilization from the bone marrow to the tumor site by VEGF, VEGF-R2, fibroblast growth factor (FGF), platelet-derived growth factor (PDGF) and stromal-derived growth factor-1 (SDF-1) and ii) angiogenesis by sprouting of the pre-existing vessels caused by increased production of VEGF, VEGF-R1, VEGF-R2, Ang-1, Ang-2, and MMPs. New blood vessels facilitate cancer cells leaving the primary tumor site, which is enhanced by increased expression of lysyl oxidase (LOX), carbonic anhydrase IX (CAIX), MMPs, integrins, and CXCR4. Hypoxic cancer cells also undergo epithelial-to-mesenchymal transition (EMT) acquiring plastic and mobile phenotype by increasing transcription factors such as Slug, Snail, and Twist and decreasing expression of adhesion molecules such as β-catenin and E-cadherin (E-cad). Chemo- and radio-resistance of patients is caused by EMT-related stemness of cancer cells and hypoxia-induced cell cycle arrest in G1 phase. Hindered drug diffusion due to anomalous vascularity is another mechanism of chemoresistance.