
Figures & data
Figure 1 This figure shows the geographic locations of the Local Health Districts within Sydney. Reproduced from © State of New South Wales NSW Ministry of Health under the Creative Commons Attribution 4.0 licence.Citation27 The Western Renal Service comprising the Western Sydney Local Health District and the Nepean Blue Mountains Local Health District serve a population of 1.3M and a total area of 9959 square kilometres.
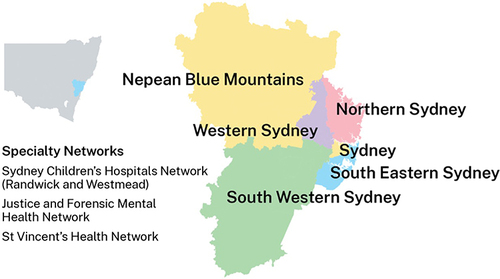
Figure 2 This figure demonstrates the standard clinical pathways for kidney failure patients in the Western Renal Service. The ideal pathway is early referral from the general practitioner to a nephrologist for pre-dialysis medical care (eg treatment with ACE/ARB inhibitors, SGTL2 inhibitors and other measures) and assessment by the pre-dialysis educator to provide education and determine the optimal renal replacement plan with a preference for encouraging home-based treatments. Planning for dialysis involves surgical referral for either the creation of a fistula for haemodialysis (including Doppler vascular mapping) or consideration of insertion of a peritoneal dialysis catheter (either by laparoscopy or the Seldinger method). Recently, there has been a marked increase in patients who present with kidney failure without a prior plan who often require insertion of a tunnelled vascular catheter for acute start haemodialysis. Additionally, these patients can commence acute dialysis through peritoneal dialysis catheter insertion using the Seldinger method. Once established on chronic dialysis, patients undergo peritoneal dialysis; or haemodialysis either in-hospital, at a satellite centre or at home. Other management pathways include kidney transplantation or renal supportive care, and importantly patients can transition between these options at any time.
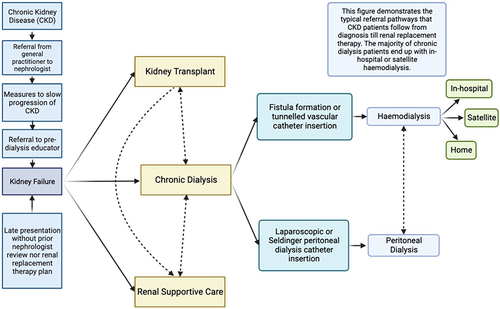
Figure 3 This figure demonstrates the factors that lead to an imbalance between an optimal healthcare system and patient satisfaction in the treatment of kidney failure. Rapid population growth in Sydney with increasing frailty multimorbidity, and cultural diversity are factors impacting service delivery in Western Sydney as well as most other high-resource healthcare systems across the world. Higher rates of sub-optimal healthcare literacy and financial disadvantage, have particularly negative impacts in the dialysis population, due to the complexity of the medical condition.
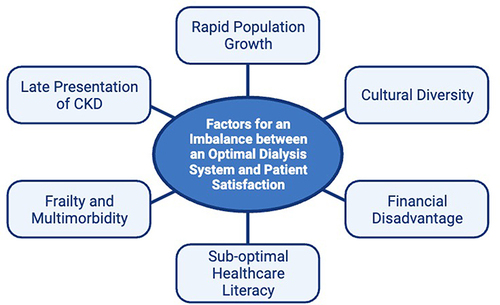
Table 1 Current Clinical Trials Addressing Symptom Management in Haemodialysis Patients