
Figures & data
Figure 1 Mechanism of action of NSAIDs.
Abbreviations: COX, cyclooxygenase; cPGES, cytosolic PGE2 synthase; CRTH2, chemoattractant receptor–homologous molecule expressed on T helper 2 cells; DP, PGD2 receptor; EP, PGE receptor; FP, PGF receptor; GI, gastrointestinal; H-PGDS, hematopoietic PGD synthase; IP, PGI2 receptor; L-PGDS, lipocalin-type PGD synthase; mPGES, membrane-associated PGE2 synthase; PG, prostaglandin; PGFS, PGF synthase; PGIS, PGI2 synthase; tNSAIDs, traditional non-steroidal anti-inflammatory drugs; TP, TX receptor; TxA2, thromboxane A2; TXS, thromboxane synthase.
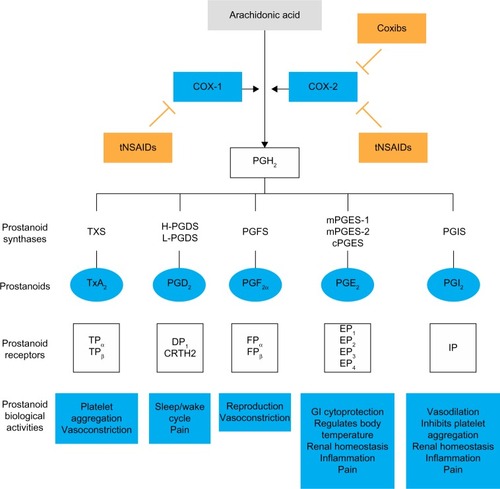
Figure 2 Selectivity of NSAIDs for COX-1 and COX-2.
Abbreviations: ASA, acetylsalicylic acid; COX, cyclooxygenase; IC50, half-maximal inhibitory concentration; NSAID, non-steroidal anti-inflammatory drug; PGI-M, 2,3-dino-6-keto-prostaglandin F1α; TxA2, thromboxane A2.
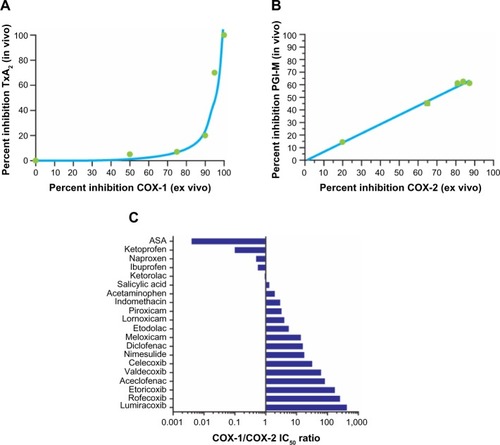
Figure 3 Average inhibition of whole-blood COX-2 activity (A) and COX-1 activity (B) by NSAIDs. Inhibition was observed over 8 hours following dosing with different NSAIDs.
Abbreviations: BID, twice-daily dosing; COX, cyclooxygenase; NSAID, non-steroidal anti-inflammatory drug; PGE2, prostaglandin E2; QD, once-daily dosing; TID, dosing three times per day; TxB2, thromboxane B2.
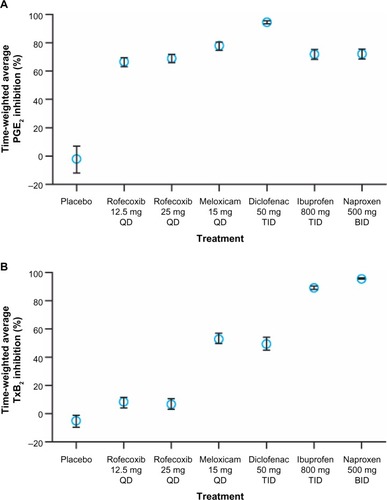
Figure 4 NSAID concentration in inflamed tissue/synovial fluid and plasma.
Abbreviations: COX, cyclooxygenase; NSAID, non-steroidal anti-inflammatory drug.
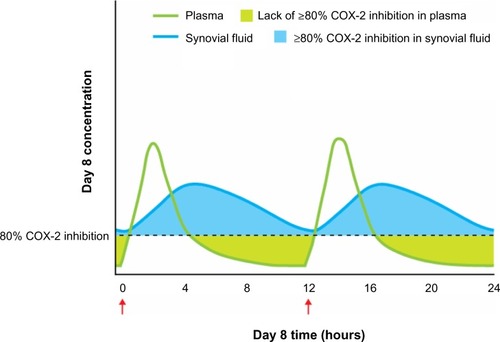
Figure 5 Predicted annual absolute risks of major vascular events or upper gastrointestinal complications with long-term, high-dose therapy.
Abbreviations: COX, cyclooxygenase; NSAIDs, non-steroidal anti-inflammatory drug; pa, per annum; SE, standard error.
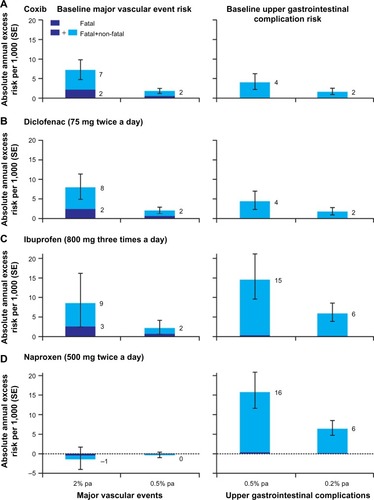
Figure 6 Determinants and sources of variability in the individual response to an NSAID.
Abbreviations: ASA, acetylsalicylic acid; COX, cyclooxygenase; CV, cardiovascular; CYP, cytochrome enzymes; GI, gastrointestinal; NSAID, non-steroidal anti-inflammatory drug; PU, peptic ulcer; SNP, single-nucleotide polymorphism.
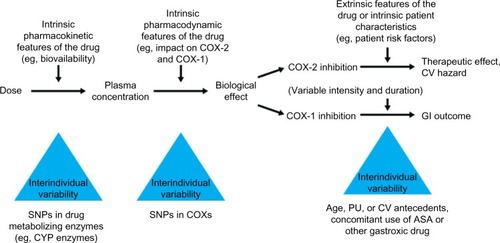
Table 1 Risk factors for NSAID gastrointestinal and cardiovascular side effects
Table 2 Prevention strategies in patients with cardiovascular and/or gastrointestinal risk factors treated with NSAIDs