Figures & data
Table 1 Percentage of Double Positive Test (PROFILE1014 and ALEX) from Retrospective Analysis of Central Labs
Table 2 Comparison of Efficacy of Crizotinib (PROFEILE 1014) and Alectinib (ALEX) per Retrospective Analysis of Central Laboratory Analysis by FISH and IHC
Figure 1 Graphic depiction of the increasing capacities of successive generation of ALK TKI being developed including the anticipated capacities of a prototypic 5th-generation (5G) ALK TKI to overcome anticipated resistances to current approved or investigational ALK TKIs.
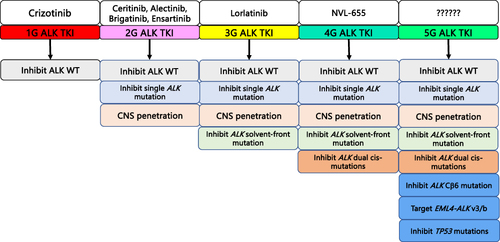
Figure 2 Continued.
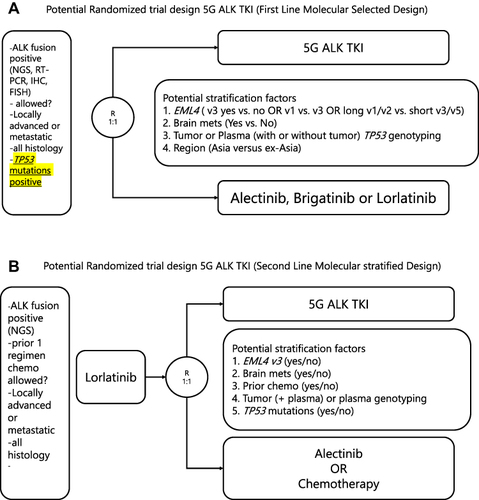
Figure 2 Hypothetical designs of pivotal randomized trials of a hypothetical 5th generation ALK TKI.
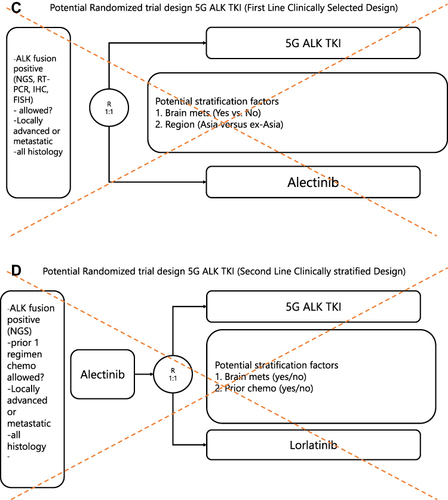
Notes: (A) Hypothetical design of a pivotal randomized molecular-selected phase 3 first-line trial of a 5G ALK TKI versus alectinib, brigatinib, or lorlatinib with ALK+ NSCLC patients harboring TP53 mutations. This design addresses the unmet need of TP53 mutations and EML4-ALK short variants (v3 and v5). Design of this first-line (1L) randomized trial will require the concurrent development of a companion diagnostic test for TP53 mutations and detection of EML4-ALK variants. This trial design is feasible given the median PFS of ALK+ NSCLC patients with TP53 mutations treated with lorlatinib is about 20 months and about 16-18 months with brigatinib and alectinib. hence the statiscal power is to be superior to ~20 months of PFS. (B) Hypothetical design of a pivotal molecularly stratified randomized phase 3 second-line (2L) trial of a 5G ALK TKI post first-line lorlatinib with ALK+ NSCLC patients. This design built upon using the most potent ALK TKI lorlatinib upfront and not the most popular ALK TKI alectinib upfront. Although no ALK TKI has been approved in the post 1L lorlatinib setting, alectinib can theoretically overcome ALK L1256F mutation. Alternate treatment option for the control arm will be platinum-pemetrexed chemotherapy. (C) Hypothetical design of an unsatisfactory clinically selected design of a pivotal 1L phase 3 trial comparing alectinib with 5G ALK TKI for all comers given PFS which did not address the poor prognostic subset of patients with TP53 mutations or “short form” of EML4-ALK variants (EML4-ALK v3 or v5). Furthermore, the median PFS of alectinib is shorter than the projected PFS achieved by lorlatinib in CROWN. Thus being superior to alectinib does not advance the holistic treatment paradigm for ALK+ NSCLC patients. This trial design is soley conduit for approval of a 5G ALK but lorlatinib will have proven far superior than alectinib. Thus developing a similar ALK drug without ddressing the true unmet need of current ALK+ NSCLC patients is suboptimal. (D) Hypothetical design of an unsatisfactory clinically selected design of a pivotal 2L phase 3 trial comparing with sequencing of alectinib to lorlatinib versus sequencing alectinib to a 5G ALK TKI. While given the median PFS of lorlatinib post-alectinib is about 5.5 months a 5G ALK TKI should be able to win over lorlatinib but even if the median PFS is triple the median PFS of lorlatinib the cumulative median PFS (26 + 16.5) will still be shorter than the projected 1L lorlatinib of > 60 months.