
Figures & data
Figure 1 Anterior approach to a Quadratus Lumborum Block. Local anaesthesia is injected under ultrasound guidance and aseptic precautions to a space between the Psoas Major Muscle and Quadratus Lumborum Muscle (Abbreviations EOM: External Oblique Muscle; IOM: Internal Oblique Muscle; TAM: Transversus Abdominis Muscle; PM: Psoas Major Muscle; ES: Erector Spinae Muscle; QL: Quadratus Lumborum Muscle; LD: Latissimus Dorsi Muscle; TP: Vertebral Body Transverse Process). ©2023 Body Scientific International, LLC.
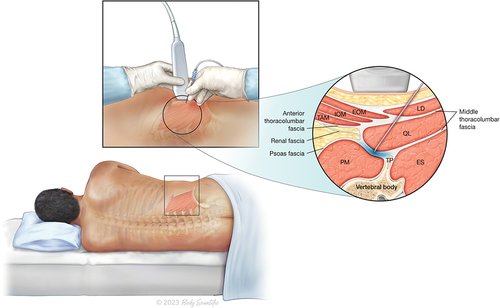
Figure 2 Clinical care pathway for our patient taking into consideration guidelines and recommendations for management of a cardiac patient presenting for non-cardiac surgery from the American Heart Association, American College of Cardiology, European Society of Cardiology and Canadian Cardiovascular Society. Additionally, we used input from a multidisciplinary team meeting with the surgical team and senior anaesthetists to make our decision. The black ticks highlight our steps in each phase of the patient’s care.
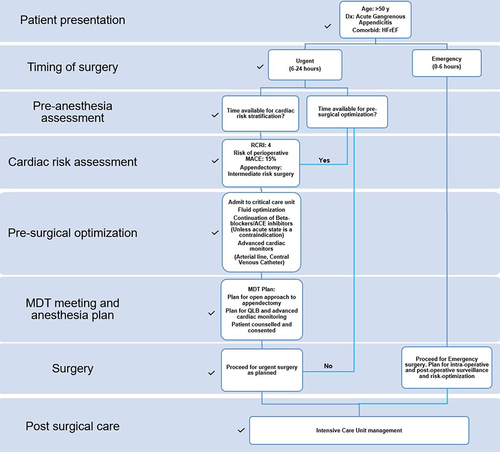
Figure 3 Pain type, intensity and distribution in Appendicitis patients. Acute appendicitis (top left) mainly produces well-localized sharp pain (red color overlay) in the left lower abdomen, with referred pain to the umbilicus (yellow color overlay), which is more poorly localized. Open appendectomy (top middle) produces sharp incisional pain in addition to pain associated with acute appendicitis (red overlay). Further pain occurs during blunt dissection of deeper muscles and tissues, and visceral pain occurs during peritoneal incision and appendix manipulation. Laparoscopic appendectomy (top right) produces sharp incisional pain at the sites of trocar insertion in addition to the pre-existing pain of acute appendicitis (red overlay). After carbon dioxide insufflation, diffuse stretching of the abdomen and peritoneum results in diffuse and poorly localized discomfort (green overlay). There is also referred pain in the shoulder due to irritation of the diaphragm (green overlay). ©2023 Body Scientific International, LLC.
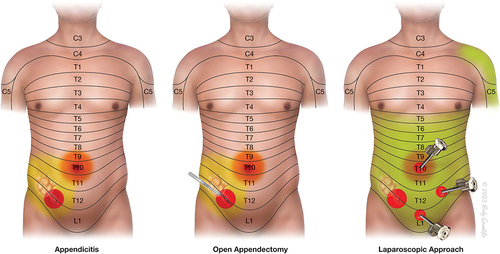
Figure 4 Anesthetic coverage by a well performed Quadratus Lumborum block providing adequate coverage of the pain of open appendectomy (blue overlay). However, some amount of visceral pain is not completely blocked. ©2023 Body Scientific International, LLC.
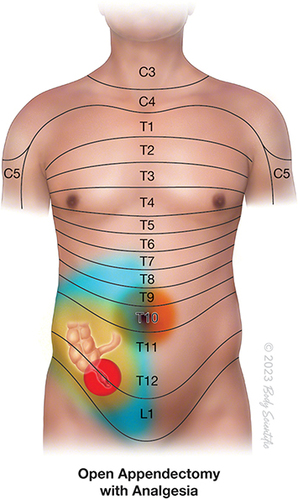
Table 1 Summary of Case Reports of Quadratus Lumborum Block as Anesthetic Technique for Abdominal Surgeries