Figures & data
Figure 1. Preoperative and postoperative MRI imaging.
Preoperative mid-sagittal (A) and coronal (B) postcontrast T1 WI showing a lobulated solid enhancing 3rd intraventricular mass, displacing the optic chiasm (Ch) downwards and forwards, bowing the floor of the third ventricle (3V) and sparing the pituitary stalk, infundibulum and the chiasmatic cistern (Ch cs), associated with subsequent obstructive hydrocephalus (asterisks). Serial mid-sagittal postcontrast T1 WI images (C) immediately following debulking of the 3rd intraventricular mass showing residual enhancing component (arrow) and resolution of the hydrocephalus (asterisks), (D) significant progression of the mass without treatment on the 4-month postoperative follow-up scan. Vemurafenib and cobimetinib combination therapy was started within 2 weeks and the 3-month post combination therapy shows significant reduction in the size of the residual mass (E). (F) 11-days after the treatment is held, the residual mass continues to shrink and show cavitary changes. Most recent mid-sagittal (G) and coronal (H) postcontrast T1 WI showing near complete resolution of the mass with a subcentimetric residual enhancing focus which remained stable for 1 year since it attained this size (85 weeks since treatment was withheld).
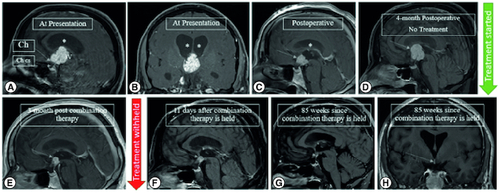
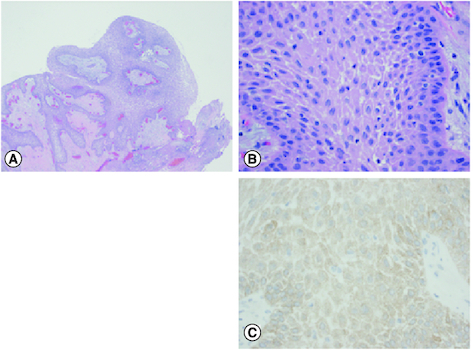
Figure 2. Histopathological findings.
Histopathology of the tumor, with H&E histology at 40× magnification (A), 400× magnification (B) and BRAF V600E immunohistochemistry at 400× magnification (C).
An epithelium-lined mass with papillary configuration is noted (A) consisting of well-differentiated stratified squamous epithelium (B) overall similar to the appearance of a squamous papilloma, and in this anatomic location, characteristic of a papillary craniopharyngioma. Mutation specific immunohistochemistry for BRAF V600E was positive (C), also typical of papillary craniopharyngioma.