Figures & data
Figure 1. (a). Portovenous phase axial CT pancreas with oral and IV contrast at the time of the initial diagnosis. The CT shows a 2.5 cm exophytic mass arising from the uncinate process of the pancreas (white arrow) which abuts, but does not encase, the superior mesenteric vein and artery (broken arrow). The mass is contiguous with the third part of the duodenum (arrow head). (b). Portovenous phase axial CT pancreas with oral and IV contrast. Following treatment with concurrent gemcitabine and radiotherapy, the mass has decreased in size measuring 2 cm (white arrow). There is now a definitive fat plane between the pancreatic lesion and the third part of the duodenum (arrow head). The tumour abuts but does not encase the superior mesenteric vein and artery (broken arrow). A biliary drain can be seen in the duodenum.
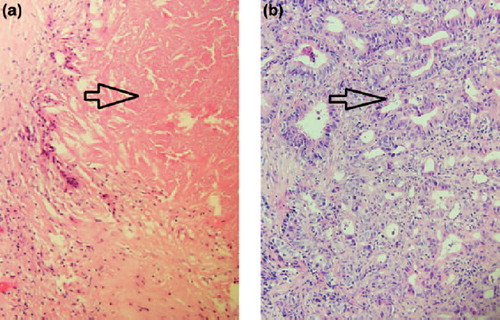
Figure 2. (a). Tumour biopsy pre-conversion therapy. (40×). Invasive adenocarcinoma is arrowed. (b). Lymph node from resection specimen post-conversion therapy. Extensive treatment effect including fibrosis has obliterated normal lymph node architecture. Necrosis (arrowed) is present, consistent with treated tumour and is associated with palisaded giant cell reaction. (40×).