
Figures & data
Figure 1. Illustration of the conversion function between the PET uptake and the dose prescription. The histogram of the uptake from Patient 1 is shown on the lower panel. The conversion takes into account bounds along both axes. The uptake bounds are given by statistics observed in the tumor volume. In the proposed solution, the minimum is overlooked, as it is likely to be contaminated by the colder background (spill in/spill out effect). Instead, the baseline uptake in the tumor is approximated by the median uptake, which is less sensitive to hot spots than the mean. The dose is interpolated linearly up to the maximum uptake in absence of further information.
Figure 2. Design of the dose adaptation procedure. Separate image sets (pre-treatment and after 5, 10 and 15 fractions of RT) were acquired for each planning phase. Using deformable image co-registration, volumes-of-interest (CTVs and OARs) were deformed from one CT to the next and manually adjusted when needed. A PTVPET and sub-contours for DP were created from each new PET image and incorporated to the deformed CTVs and OARs. For each phase, a new treatment plan was made. Dose summation was performed anti-chronologically on the pretreatment PET-CT.
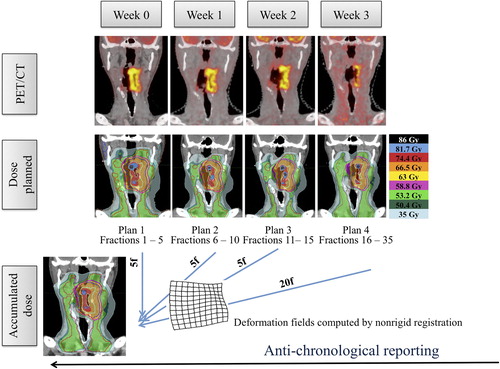
Table I. QVH metrics (VQ = 0.95, VQ = 1.05, QF, %) calculated for the dose-painted PTVPET on pre-treatment images with a number of sub-contours increasing from 3 to 9 (jaw width 1 cm, pitch 0.43, planned MF of 3 corresponding to a mean actual MF of 2.49 ± 0.27).
Table II. Volume of the gross tumor volume (GTVPET) on consecutive PET/CT scans.
Table III. Dose/volume parameters for targets and organs-at-risk for pre-treatment CT and dose accumulation. Population-average doses (mean± SD) are reported in volumes-of-interest on pre-treatment CT.
Table IV. QVH metrics (VQ = 0.95, VQ = 1.05, QF, %) calculated for the dose-painted PTVPET on per-treatment PET-CT scans with anatomic adaptation versus molecular and anatomic adaptation.