Figures & data
Table I. TNM classification (version 5, 1997) with subclassifications.
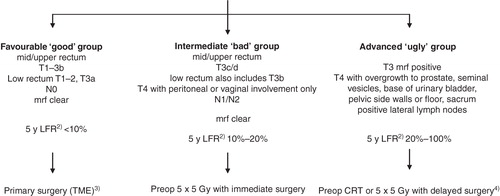
Figure 1. Subgrouping of localized rectal cancer assessed by MRI 1) and recommended primary treatment. 1)The algorithm does not primarily address the risk of systemic disease, although this risk also increases with the presence of many of ‘the risk factors’, however, not necessarily parallel to the local failure rate (LFR). The algorithm is also ‘too simplified’ in that also other factors like size of the mesorectum, anterior or posterior location, extramural vascular invasion (EMVI+) are relevant. The recommendations are the ones in use at most centres in Sweden in 2011. 2)Calculated in the group of patients planned for surgery, i.e. irrespective of the surgical outcome. The figures are valid if the surgeon is an experienced rectal cancer surgeon and no pretreatment is given. 3)A local procedure is possible in a few patients (chiefly pT1, sm1 (+2), N0). This group is in the text referred to as ‘very favourable’. 4)CRT means chemoradiotherapy to 50.4 Gy in 1.8 Gy fractions with 5-fluorouracil (capecitabine); 5 × 5 Gy with delayed surgery is used in patients not fit for CRT.