
Figures & data
Table I. Classification of angioedema (modified from Caballero et al. (Citation49)).
Figure 1. Schematic diagram showing type I hypersensitivity reactions.
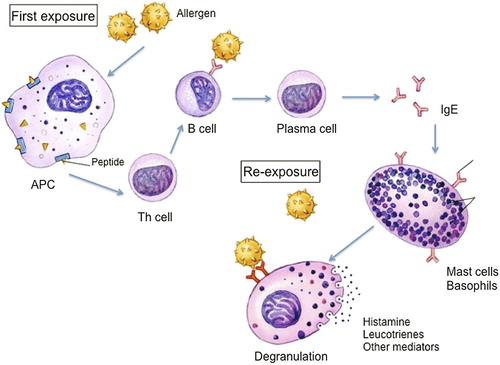
Figure 2. The contact system, showing the generation and degradation of bradykinin (reproduced with permission from: Caballero T, et al. J Investig Allergol Clin Immunol. 2011;21:333–47). ACE = angiotensin-converting enzyme; APP = aminopeptidase P; B1R = bradykinin B1 receptor; B2R = bradykinin B2 receptor; C1-INH = C1 esterase inhibitor; HMWK = high-molecular-weight kininogen; LMWK = low-molecular-weight kininogen; tPA = tissue plasminogen activator; UK = urokinase.
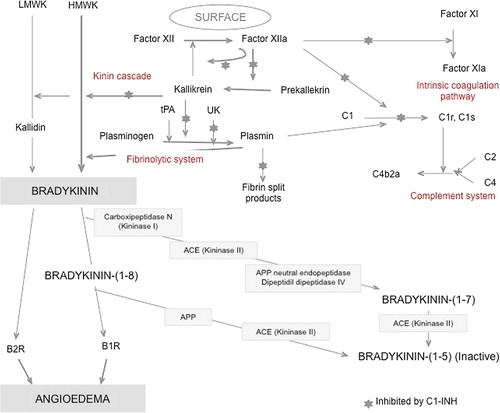
Table II. Differential features of bradykinin and histamine-mediated angioedema.
Figure 3. The picture shows an erythema marginatum preceding an angioedema acute attack in a patient with type I HAE. The erythematous rash with circular polycyclic border and a clear center should not be confused with urticaria.

Table III. Staging system of airway obstruction risk from Ishoo et al. (Citation58).
Figure 4. Algorithm for management of acute angioedema in the emergency department. Note: Non-responders are considered when there is not an improvement 30–60 minutes after antihistamines, steroids, and/or epinephrine treatment. *Doses and treatment in each type of angioedema as described in . In those cases that a patient with ACEi treatment presents the first attack of angioedema, and the localization or the history of the evolution of the angioedema does not seem to be related to ACEi, first it is preferred to treat with antihistamines, steroids, and epinephrine to confirm that it is a histamine-mediated angioedema or it is a bradykinin angioedema. **In those cases that patient has presented previous episodes of angioedema without response to antihistamines, steroids, and epinephrine, or in those cases that suspicion of ACEi induced angioedema is elevated, they should be treated directly as a bradykinin-mediated angioedema as shown in . Indications for treatment of acute episodes depend on the severity and location of the angioedema episodes. One should treat all episodes of glottic edema, those that affect the cervicofacial or pharyngolaryngeal region, and also abdominal episodes. Peripheral episodes should be treated based on the impact on the patient's quality of life. HAE = hereditary angioedema; ACEI = angiotensin-converting enzyme inhibitors; ICU = intensive care unit.
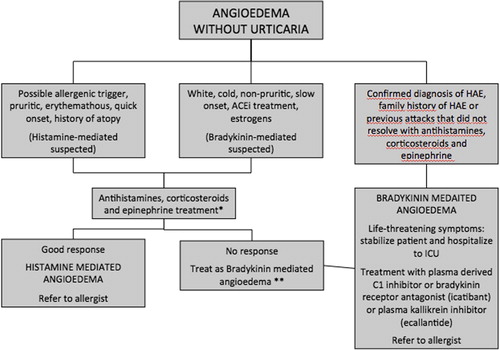
Table IV. Treatment profile in each type of angioedema.