
Figures & data
Figure 1. The developing heart; contributions from the second heart field. a: Primary heart tube, consisting mainly of the putative left ventricle (LV) and only very limited parts of the inflow tract (atria, sinus venosus) and outflow tract of the heart. The myocardium of the primary heart tube is derived from the splanchnic mesoderm of the primitive plate, the so-called ‘first heart field’ (FHF). Fetal blood enters the blood at the venous pole, and via peristaltic movements is propelled to the arterial pole of the heart tube. The tube consists at this stage of endocardial and myocardial cells (depicted in grey), with cardiac jelly (CJ, depicted in blue) in between. No epicardial covering is present at this stage. b: The heart tube after looping has been initiated. The tube is now U-shaped. The inner curvature is indicated by an asterisk and is continuous with the bulboventricular or primary fold (arrow) that encircles the heart tube between the primitive left ventricle (“LV”) and primitive right ventricle (“RV”). FHF-derived parts of the myocardium are depicted in grey. In addition, myocardium has been recruited to the arterial and venous heart tube from the mesenchyme situated behind the heart during development, the so-called ‘second heart field’ (SHF, also see panel d). SHF-derived structures are depicted in yellow. The CJ has concentrated at the AV canal (AVC) and outflow tract (OFT) to the endocardial cushion (EC) and will contribute to, for example, the cardiac valves during further development. The venous pole consists of the right cardinal vein (RCV, putative superior caval vein), left caval vein (LCV, that will form part of the putative coronary sinus), and vitelline veins entering the tube. Atrial and ventricular septation have not occurred, yet. The blood from the common atrium (A) passes through the AVC into “LV”, and via the interventricular foramen to the primitive right ventricle “RV” and OFT. The latter is initially positioned entirely above the “RV”. c: Situation after atrial and ventricular septation has been completed. A right atrium (RA) to RV connection has now been formed by an expansion of the AV canal to the right side, thus forming the tricuspid ostium. The OFT has been separated into an aorta (Ao) connecting to the LV and a pulmonary trunk (PT) still connecting to the RV. SHF-derived myocardium is depicted in yellow. d:Scheme of the embryo (lateral view) demonstrating the cellular contributions to the heart. The SHF mesenchyme is depicted in yellow, as are structures derived from this mesenchyme. SHF contributing to the arterial pole of the heart is referred to as ‘anterior SHF’, whereas cells are recruited to the venous pole from the ‘posterior SHF’. The pro-epicardial organ (PEO), that is present at both the venous (vPEO) and arterial (aPEO) pole of the heart (Citation33), is also derived from the SHF. Neural crest cells (NCC, indicated by dark blue dots) reflect an extracardiac contribution to the heart. For additional explanation see text. (AoS = aortic sac; CV = cardinal vein; DA = ductus arteriosus; ICV = inferior caval vein; LA = left atrium; LVV = left venous valve; PAA = pharyngeal arch arteries; PV = primitive pulmonary vein; SCV = superior caval vein; RVV = right venous valve).
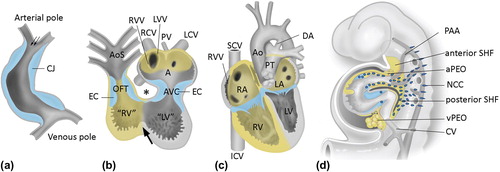
Figure 2. Atrial septation. a: Early developmental stage. Atrial septation starts with formation of a muscular septum primum (SP), that grows out from the roof of the atrium towards the AV canal (AVC). The lower rim of the SP consists of mesenchymal tissue, the mesenchymal cap (MC, indicated in dark blue) that is continuous with the endocardial cushions in the AV canal (light blue). Initially, the lower part of the SP will not connect to the tissues in the AV canal, leaving an opening, the ostium primum (OP). b: During further development, the OP will be closed by fusion of the endocardial cushion with the mesenchymal cap, as well as with second heart field (SHF) mesenchyme protruding into the heart at the base of the atrial septum. This protrusion is referred to as dorsal mesenchymal protrusion (DMP). Meanwhile, the ostium secundum (OS) in the muscular SP has developed by a process of apoptosis. The septum secundum (SS) is formed at the right side of the SP by an infolding of the roof of the atrium, but will never entirely reach the AVC. The free rim of the septum secundum forms the limbus of the foramen ovale. During the entire fetal phase the foramen ovale (consisting of the opening between the lower rim (limbus) of the SS and the OS secundum) will allow shunting of blood from the right atrium (RA) to the left atrium (LA) (arrow in panel b). c: Schematic overview of the three structures responsible for proper closure of the OP during development: the atrioventricular endocardial cushions (EC, light blue), the mesenchymal cap (MC, dark blue), and the dorsal mesenchymal protrusion (DMP, yellow). d–f: Transverse sections stained with the myocardial marker myosin light chain 2a (MLC2a) of murine embryonic wild-type hearts, stage E12.5. d. is the most superior and f. the most inferior section. Elements contributing to normal atrial septation are indicated. (AS = atrial septum; LV = left ventricle; LCV = left cardinal vein; LVV = left venous valve; MO = mitral ostium; PV = pulmonary vein; TO = tricuspid ostium; RV = right ventricle; RVC = right cardial vein; RVV = right venous valve; VS = ventricular septum). a and b: modified after (Citation116).
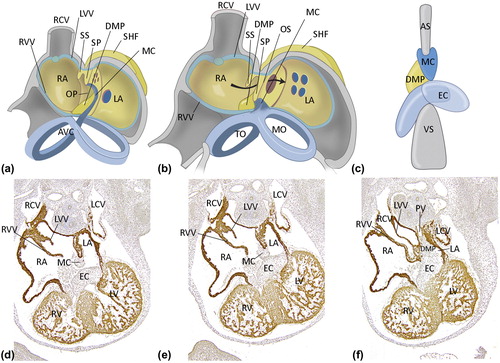
Figure 3. Ventricular septation. a: Schematic overview of ventricular septation. Remodeling of the primary fold (PF) is essential for the formation of the right ventricular (RV) inlet compartment and positioning of the right side of the AV canal (AVC) above the RV, which will result in formation of the tricuspid orifice (TO). The mitral orifice (MO) will remain above the left ventricle (LV). Formation of the TO and MO is achieved by fusion of the atrioventricular endocardial cushions (indicated in pale blue). The anterior trabeculated part of the ventricular septum (TS) derives from infolding of the anterior part of the primitive ventricle, whereas the inlet septum (IS) and inlet cavity of the RV are formed by expansion of the posterior part of the PF. The borderline between the RV inlet compartment and folding septum is visible as the septal band (SB). b and c: In the outflow tract (OFT), the endocardial cushions (indicated in pale blue) fuse to separate the left and right ventricular OFT in an aorta (Ao) and pulmonary trunk (PT). During normal septation, neural crest cells migrate into the cushions and orchestrate the formation of an OFT septum before they go into apoptosis (not shown). At the ventricular level, the primary interventricular foramen (double arrow) is still patent but will be closed with completion of OFT septation and connection of the Ao to the LV. (ICV = inferior caval vein; LA = left atrium; LV = left ventricle; MO = mitral orifice; SCV = superior caval vein; RA = right atrium; TO = tricuspid orifice). Modified after: Crawford Cardiology (Citation117).
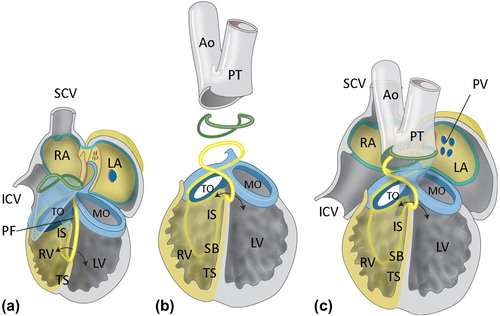
Figure 4. The cardiac septa in the adult and morphology of septal defects. a: Normal atrial septum after birth, right lateral view. A fenestration has been drawn to allow visualization of the atrial septum. The foramen ovale is closed and can be recognized as the fossa ovalis (FO). b: Patent foramen ovale, as seen from the left atrium (LA). The valvula foraminis ovalis (VFO, derived from the embryological septum primum) is competent but has not fused with the septum secundum, thus allowing the probe to be inserted from the right side. c: Atrial septal defect type 2, as viewed from the right atrium (RA). The valvula foraminus ovalis (VFO, septum primum) is deficient, thus leaving a septum defect (arrow). d: Normal ventricular septum, as viewed from the right side. The different septal components can be recognized and include the ventricular inlet septum (IS), below the tricuspid orifice, and the anterior and apical trabeculated parts (TS). The septal band (SB) and moderator band (MB, which has been cut in order to open the RV) are indicated. e: Perimembranous ventricular septal defect (arrow), as seen from the right ventricle (RV). f: Central muscular ventricular septal defect (arrow), as seen from the left ventricle (LV). The defect is classically situated at the border between two septal components, i.e. the inlet septum (IS) and the trabeculated septum (TS). g: Normal atrioventricular septum. Note the differential insertion of the tricuspid valve (TV) and mitral valve (MV), resulting in the length of the AV septum between the right atrium and left ventricle. The membranous septum consists of an atrioventricular (double arrow) and interventricular part. h: Complete AVSD. The anterior bridging leaflet (ABL) and inferior bridging leaflet (IBL) are not attached to the atrial septum (not shown) and ventricular septum (VS), allowing shunting at both the atrial and ventricular level. i: Incomplete AVSD. Both the superior bridging leaflet (SBL) and inferior bridging leaflet (IBL) are attached to the ventricular septum (VS), therefore shunting can only occur at the atrial level (not shown). (CS = coronary sinus; ICV = inferior caval vein; ML = mural leaflet; MV = mitral valve; PV = pulmonary veins; PuV = pulmonary valve; RVV = right venous valve; SCV = superior caval vein; VS = ventricular septum).
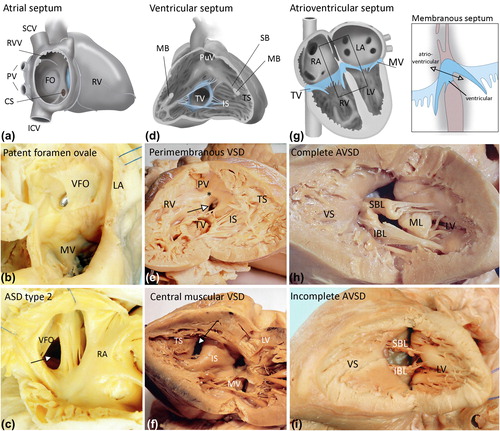
Table I. Genes encoding for transcription factors and proteins related to human congenital heart disease. Special attention is given to the NODAL (Δ) and the VEGF pathways (*).
Figure 5. Overview of genes involved in cardiac septation. Modified after (Citation2).
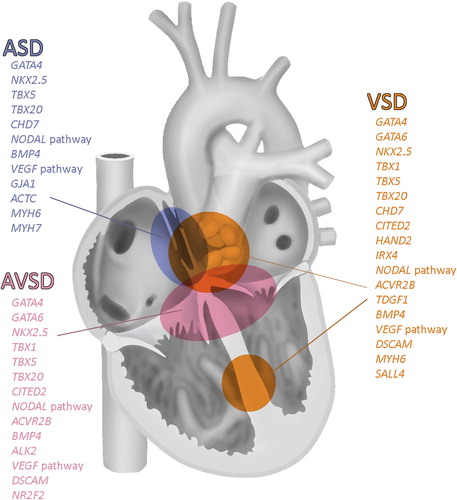
Table II. Syndromes associated with congenital heart disease with mutation in genes that are linked to the SHH pathway.