2013 ESH/ESC Guidelines for the management of arterial hypertension
The Task Force for the management of arterial hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC)
Giuseppe ManciaESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).Correspondence[email protected][email protected]
,
Robert FagardESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).Correspondence[email protected][email protected]
,
Krzysztof NarkiewiczDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Josep Redon The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
,
Alberto ZanchettiESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
,
Michael BöhmESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).
,
Thierry ChristiaensDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Renata Cifkova The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
,
Guy De BackerESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
,
Anna DominiczakESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).
,
Maurizio GalderisiDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Diederick E. Grobbee The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
,
Tiny JaarsmaESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
,
Paulus KirchhofESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).
,
Sverre E. KjeldsenDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Stéphane Laurent The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
,
Athanasios J. ManolisESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
,
Peter M. NilssonESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).
,
Luis Miguel RuilopeDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Roland E. Schmieder The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
,
Per Anton SirnesESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
,
Peter SleightESC Committee for Practice Guidelines (CPG): Jose Luis Zamorano (Chairperson) (Spain), Stephan Achenbach (Germany), Helmut Baumgartner (Germany), Jeroen J. Bax (Netherlands), Héctor Bueno (Spain), Veronica Dean (France), Christi Deaton (UK), Cetin Erol (Turkey), Robert Fagard (Belgium), Roberto Ferrari (Italy), David Hasdai (Israel), Arno W. Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Patrizio Lancellotti (Belgium), Ales Linhart (Czech Republic), Petros Nihoyannopoulos (UK), Massimo F. Piepoli (Italy), Piotr Ponikowski (Poland), Per Anton Sirnes (Norway), Juan Luis Tamargo (Spain), Michal Tendera (Poland), Adam Torbicki (Poland), William Wijns (Belgium), Stephan Windecker (Switzerland).
,
Margus ViigimaaDocument Reviewers: Denis L. Clement (ESH Review Co-ordinator) (Belgium), Antonio Coca (ESH Review Co-ordinator) (Spain), Thierry C. Gillebert (ESC Review Co-ordinator) (Belgium), Michal Tendera (ESC Review Co-ordinator) (Poland), Enrico Agabiti Rosei (Italy), Ettore Ambrosioni (Italy), Stefan D. Anker (Germany), Johann Bauersachs (Germany), Jana Brguljan Hitij (Slovenia), Mark Caulfield (UK), Marc De Buyzere (Belgium), Sabina De Geest (Switzerland), Geneviève Anne Derumeaux (France), Serap Erdine (Turkey), Csaba Farsang (Hungary), Christian Funck-Brentano (France), Vjekoslav Gerc (Bosnia & Herzegovina), Giuseppe Germano (Italy), Stephan Gielen (Germany), Herman Haller (Germany), Arno W. Hoes (Netherlands), Jens Jordan (Germany), Thomas Kahan (Sweden), Michel Komajda (France), Dragan Lovic (Serbia), Heiko Mahrholdt (Germany), Michael Hecht Olsen (Denmark), Jan Ostergren (Sweden), Gianfranco Parati (Italy), Joep Perk(Sweden), Jorge Polonia (Portugal), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Lars Rydén (Sweden), Yuriy Sirenko (Ukraine), Alice Stanton (Ireland), Harry Struijker-Boudier (Netherlands), Costas Tsioufis (Greece), Philippe van de Borne (Belgium), Charalambos Vlachopoulos (Greece), Massimo Volpe (Italy), David A. Wood (UK).
,
Bernard Waeber The affiliations of the Task Force Members are listed in the Appendix. The disclosure forms of the authors and reviewers are available on the respective society websites http://www.eshonline.org and www.escardio.org/guidelines
&
Faiez ZannadESH Scientific Council: Josep Redon (President) (Spain), Anna Dominiczak (UK), Krzysztof Narkiewicz (Poland), Peter M. Nilsson (Sweden), Michel Burnier (Switzerland), Margus Viigimaa (Estonia), Ettore Ambrosioni (Italy), Mark Caufield (UK), Antonio Coca (Spain), Michael Hecht Olsen (Denmark), Roland E. Schmieder (Germany), Costas Tsioufis (Greece), Philippe van de Borne (Belgium).
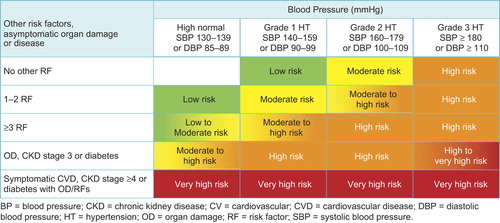
Figure 1. Stratification of total CV risk in categories of low, moderate, high and very high risk according to SBP and DBP and prevalence of RFs, asymptomatic OD, diabetes, CKD stage or symptomatic CVD. Subjects with a high normal office but a raised out-of-office BP (masked hypertension) have a CV risk in the hypertension range. Subjects with a high office BP but normal out-of-office BP (whitecoat hypertension), particularly if there is no diabetes, OD, CVD or CKD, have lower risk than sustained hypertension for the same office BP.
Table IV. Factors—other than office BP—influencing prognosis; used for stratification of total CV risk in .
Table XI. Cut-off values for parameters used in the assessment of LV remodelling and diastolic function in patients with hypertension. Based on Lang et al.Citation158 and Nagueh et al.168.
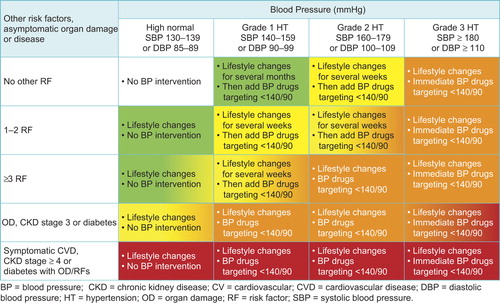
Figure 2 Initiation of lifestyle changes and antihypertensive drug treatment. Targets of treatment are also indicated. Colours are as in . Consult Section 6.6 for evidence that, in patients with diabetes, the optimal DBP target is between 80 and 85 mmHg. In the high normal BP range, drug treatment should be considered in the presence of a raised out-of-office BP (masked hypertension). Consult section 4.2.4 for lack of evidence in favour of drug treatment in young individuals with isolated systolic hypertension.
Figure 3. Monotherapy vs. drug combination strategies to achieve target BP. Moving from a less intensive to a more intensive therapeutic strategy should be done whenever BP target is not achieved.
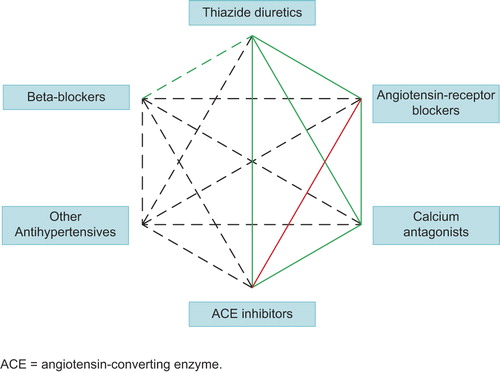
Figure 4. Possible combinations of classes of antihypertensive drugs. Green continuous lines: preferred combinations; green dashed line: useful combination (with some limitations); black dashed lines: possible but less well-tested combinations; red continuous line: not recommended combination. Although verapamil and diltiazem are sometimes used with a beta-blocker to improve ventricular rate control in permanent atrial fibrillation, only dihydropyridine calcium antagonists should normally be combined with beta-blockers. ACE: angiotensin-converting enzyme.
Cuspidi C, Ambrosioni E, Mancia G, Pessina AC, Trimarco B, Zanchetti A. Role of echocardiography and carotid ultrasonography in stratifying risk in patients with essential hypertension: the Assessment of Prognostic Risk Observational Survey. J Hypertens 2002;20:1307–1314.
PROGRESS Collaborative Group. Randomised trial of a perindopril-based blood-pressure-lowering regimen among 6,105 individuals with previous stroke or transient ischaemic attack. Lancet 2001;358:1033–1041.
ADVANCE Collaborative Group. Effects of a fixed combination of perindopril and indapamide on macrovascular and microvascular outcomes in patients with type 2 diabetes mellitus (the ADVANCE trial): a randomised controlled trial. Lancet 2007;370:829–840.
Beckett NS, Peters R, Fletcher AE, Staessen JA, Liu L, Dumitrascu D, Stoyanovsky V, Antikainen RL, Nikitin Y, Anderson C, Belhani A, Forette F, Rajkumar C, Thijs L, Banya W, Bulpitt CJ. Treatment of hypertension in patients 80 years of age or older. N Engl J Med 2008;358:1887–1898.
Hansson L, Lindholm LH, Niskanen L, Lanke J, Hedner T, Niklason A, Luomanmaki K, Dahlof B, de Faire U, Morlin C, Karlberg BE, Wester PO, Bjorck JE. Effect of angiotensin-converting-enzyme inhibition compared with conventional therapy on cardiovascular morbidity and mortality in hypertension: the Captopril Prevention Project (CAPPP) randomised trial. Lancet 1999;353:611–616.
Lithell H, Hansson L, Skoog I, Elmfeldt D, Hofman A, Olofsson B, Trenkwalder P, Zanchetti A. The Study on Cognition and Prognosis in the Elderly (SCOPE): principal results of a randomized double-blind intervention trial. J Hypertens 2003;21: 875–886.
Dahlof B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S,Wedel H. LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002;359:995–1003.
Liu L, Zhang Y, Liu G, Li W, Zhang X, Zanchetti A. The Felodipine Event Reduction (FEVER) Study: a randomized long-term placebo-controlled trial in Chinese hypertensive patients. J Hypertens 2005;23:2157–2172.
Zanchetti A, Bond MG, Hennig M, Neiss A, Mancia G, Dal Palu C, Hansson L, Magnani B, Rahn KH, Reid JL, Rodicio J, Safar M, Eckes L, Rizzini P. Calcium antagonist lacidipine slows down progression of asymptomatic carotid atherosclerosis: principal results of the European Lacidipine Study on Atherosclerosis (ELSA), a randomized, double-blind, long-term trial. Circulation 2002;106:2422–2427.
Black HR, Elliott WJ, Grandits G, Grambsch P, Lucente T, White WB, Neaton JD, Grimm RH Jr, Hansson L, Lacourciére Y, Muller J, Sleight P, Weber MA, Williams G, Wittes J, Zanchetti A, Anders RJ. CONVINCE Trial group. Principal results of the Controlled Onset Verapamil Investigation of Cardiovascular End Points (CONVINCE) trial. JAMA 2003;289:2073–2082.
Julius S, Kjeldsen SE,Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schrok A, Smith B, Zanchetti A. VALUE trial group.- Outcomes inhypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004;363:2022–2031.
Liu L, Wang JG, Gong L, Liu G, Staessen JA. Comparison of active treatment and placebo in older Chinese patients with isolated systolic hypertension. Systolic Hypertension in China (Syst-China) Collaborative Group. J Hypertens 1998;16:1823–1829.
Hansson L, Hedner T, Lund-Johansen P, Kjeldsen SE, Lindholm LH, Sylversten JO, Lanke J, de Faire U, Dalhof B, Karlberg BE. Randomised trial of effects of calcium antagonists compared with diuretics and beta-blockers on cardiovascular morbidity and mortality in hypertension: the Nordic Diltiazem (NORDIL) study. Lancet 2000;356:359–365.
Sarafidis PA, Lasaridis A, Gousopoulos S, Zebekakis P, Nikolaidis P, Tziolas I, Papoulidou F. Prevalence, awareness, treatment and control of hypertension in employees of factories of Northern Greece: the Naoussa study. J Hum Hypertens 2004;18:623–629.
Jamerson K, Weber MA, Bakris GL, Dahlof B, Pitt B, Shi V, Hester A, Gupte J, Gatlin M, Velazquez EJ. Benazepril plus amlodipine or hydrochlorothiazide for hypertension in high-risk patients. N Engl J Med 2008;359:2417–2428.
SHEP Co-operative Research Group.Prevention of stroke by antihypertensive drug treatment in older persons with isolated systolic hypertension. Final results of the Systolic Hypertension in the Elderly Program (SHEP). JAMA 1991;265:3255–3264.
Dahlof B, Lindholm LH, Hansson L, Schersten B, Ekbom T,Wester PO. Morbidity and mortality in the Swedish Trial in Old Patients with Hypertension (STOP-Hypertension). Lancet 1991;338:1281–1285.
Hansson L, Lindholm LH, Ekbom T, Dahlof B, Lanke J, Schersten B, Wester PO, Hedner T, de Faire U. Randomised trial of old and new antihypertensive drugs in elderly patients: cardiovascular mortality and morbidity the Swedish Trial in Old Patients with Hypertension-2 study. Lancet 1999;354:1751–1756.
ALLHAT officers and co-ordinators for the ALLHAT Collaborative Research Group. Major outcomes in high-risk hypertensive patients randomized to angiotensin-converting enzyme inhibitor or calcium channel blocker vs diuretic: The Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial (ALLHAT). JAMA 2002;288:2981–2997.
Dalhof B, Sever PS, Poulter NR, Wedel H, Beevers DG, aulfield M, Collins R, Kjeldsen SE, Kristinsson A, McInnes GT, Mehlsen J, Neminen M, O’Brien E, Ostergren J. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required vs. atenolol adding bendroflumethiazide as required in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA) a multicentre randomised controlled trial. Lancet 2005;366:895–906.
Parving HH, Brenner BM, McMurray JJV, de Zeeuw D, Haffer SM, Solomon SD. Cardiorenal endpoints in a trial of aliskiren for type 2 diabetes. N Engl J Med 2012,367,2204–2213.
If you are unable to obtain permissions via Rightslink, please complete and submit this Permissions form. For more information, please visit our Permissions help page.