Figures & data
Table 1. Clinical and laboratory features of the 20 cases of FSGS-GTL.
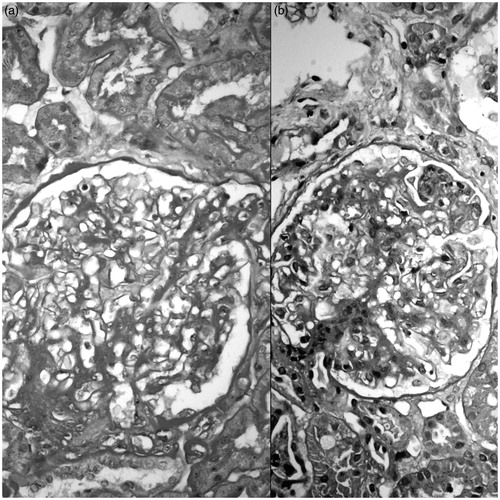
Figure 1. Sclerosed capillaries are occluded by foamy macrophages (arrows); the uninvolved parts of the glomeruli have patent capillary lumina, normal mesangium and cellularity (a: H&E × 400; b: Jones' methenamine silver × 400 (a and b depict the same glomerulus)).
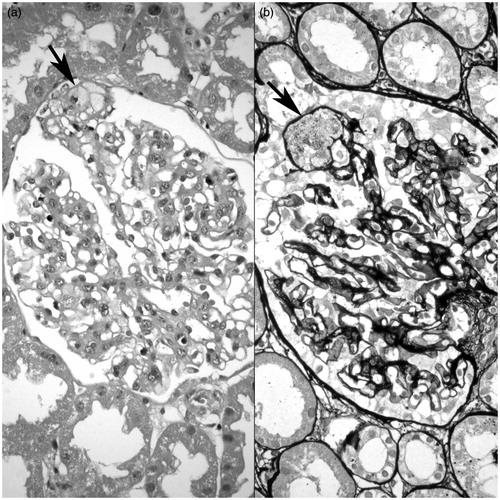
Figure 2. Sclerotic segment in each glomerulus is minute and is noted mainly by the adhesion of loop to Bowman's capsule (arrows) (a: PAS × 400; b: Masson trichrome × 400 (a and b depict the same glomerulus)).
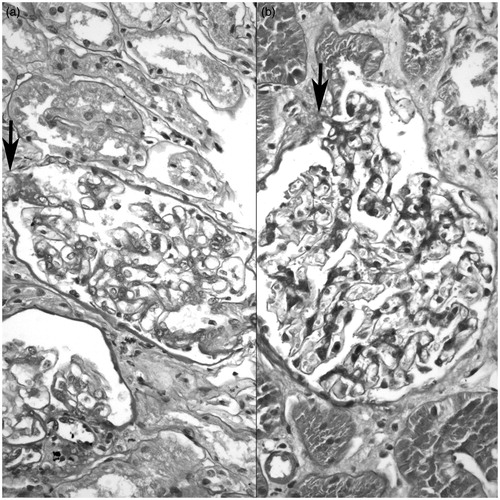
Figure 3. Tip lesions with hyalinosis (arrows) (a: H&E × 400; b: Periodic acid methenamine silver ×400 (a and b depict the same glomerulus)).
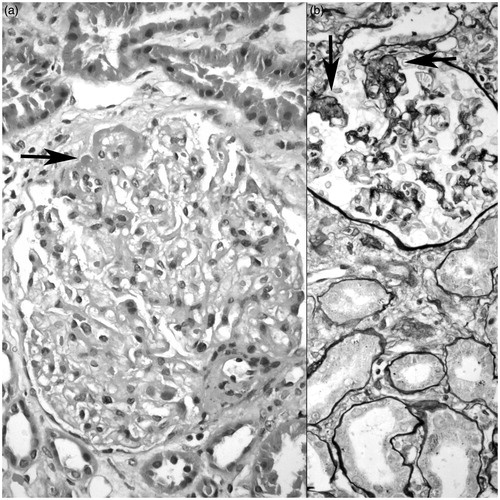
Figure 4. Glomeruli with mesangial expansion and cellularity in addition to tip lesion (a and b: PAS × 400).