Figures & data
Table 1. ECG findings described in patients with emphysema
Table 2. Patient characteristics
Figure 1. Electrocardiographic characteristics of COPD patients without and with PH.Panel A corresponds to the ECG of a COPD patient without PH (mean PAP 17 mm Hg, heart rate 81 bpm, PR interval 124 ms, QRS complex duration 76 ms, QTc interval 401 ms, QRS axis + 37° and T wave axis + 70°). Panel B shows the ECG of a COPD patient with PH (mean PAP 65 mmHg, heart rate 63 bpm, PR interval 216 ms, QRS complex duration 84 ms, QTc interval 409 ms, QRS axis + 72° and T wave axis – 22°). In the ECG of the COPD patient with PH (panel B) the PR interval (PR) is longer, the P wave (P) in V1 and the S wave in lead I are of larger amplitude. In addition, there are negative T waves in the inferior leads (*).
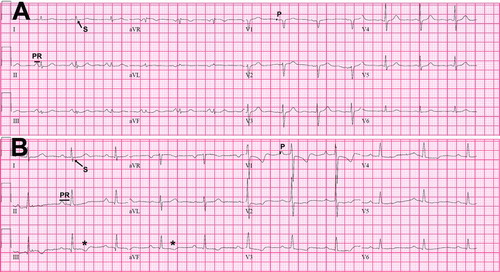
Table 3. Electrocardiographic variables
Figure 2. Hierarchical binary recursive partitioning algorithm to predict the presence of PH in COPD patients.The model correctly classified 64 out of 90 (71.1%) PH patients, and 39 out of 52 (75%) patients without PH. The model precision was 83.1% with an AUC by ROC of 0.74.
Table 4. Electrocardiographic variables in COPD patients with mean PAP < 40 or ≥ 40 mmHg
Figure 3. Hierarchical binary recursive partitioning algorithm to predict mean PAP ≥ 40 mmHg in COPD patients.The model correctly classified the 16 COPD patients (100%) with mean PAP ≥ 40 mmHg and 75 out of 126 (59.5%) patients who had a mean PAP < 40 mmHg. The model precision was 24% with an AUC by ROC of 0.80. Abbreviations: mPAP: mean pulmonary artery pressure.
Table 5. Electrocardiographic variables in COPD patients with PH and a PVR < 3 or ≥ 3 Wood Units
Figure 4. Hierarchical binary recursive partitioning algorithm to predict PAOP > 15 mmHg in COPD patients.The model correctly classified 21 out of 42 COPD patients (50%) with a PAOP > 15 mmHg and 77 out of 97 (79.4%) patients who had a PAOP ≤ 15 mmHg. The model precision was 51.2% with an AUC by ROC of 0.65. Abbreviations: PAOP: pulmonary artery occlusion pressure.