Figures & data
Figure 1. a. Lateralized left patella tendon shown through incision. * lateral fixed patellar ligament.
b. The patella tendon dissected sharply from the tibial tuberosity. Then the periosteum gets detached from the tibial crest by using a rasp (° tibial tuberosity, * patellar ligament).
c. New medialized position of the patella tendon through the incision (° tibial tuberosity, * detached patellar ligament).
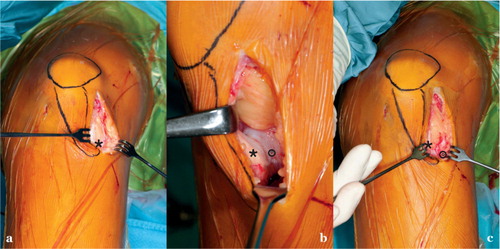
Figure 2. Schematic drawing of left knee. a. Following arthroscopy, a lateral incision was made starting at the mid-patellar level and extending distally to include the anterolateral arthroscopy portal to reach 1 cm below the tibial tuberosity. b. and c. In cases with concomitant osteochondral fragments, the incision was extended proximally allowing access to the lateral femoral condyle or the patella facet (red). Starting at the tibial tuberosity, the periosteum was split along the tibial crest for 6–8 cm distally without opening the fascia of the tibialis anterior muscle (red). The periosteum was subsequently detached from the tibial crest with a large rasp (blue). In knee flexion, the patella tendon then slides spontaneously medially to track within the femoral groove. Patella alignment was restored (green).
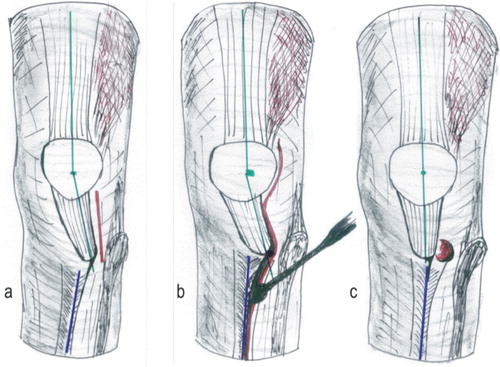
Figure 3. a. Sagittal-plane view of the proximal tibia (deep incision) indicating the relation of the patellar tendon insertion and the anterior tongue of the physis. Note that the physis remains untouched. LP: ligamentum patellae; TA: anterior tongue of the physis; Pe; periosteum. b. The patella tendon gets sharply dissected from the tibial tuberosity. The periosteum is then split along the tibial crest and detached distally by rasp. This leads to a spontaneous slide of the patella tendon medially.
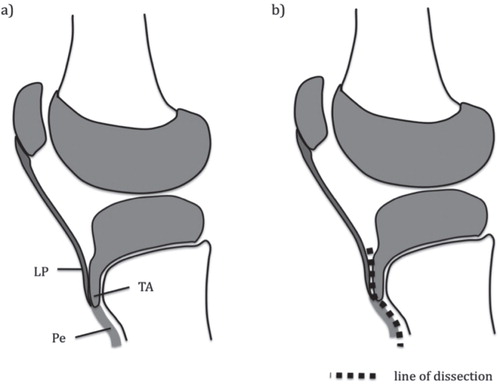
Table 1. Patient demographics and range of knee movement
Table 2. Preoperative evaluation of trochlear dysplasia
Table 3. Overview of literature