Figures & data
Figure 1. A subject carrying the Physilog system. The data logger (weighing 300 g) can be fixed around the waist. Sensors (gyroscopes) are attached by elastic strips to each shank and thigh, and also to the pelvis, and connected to the data logger by a thin cable.
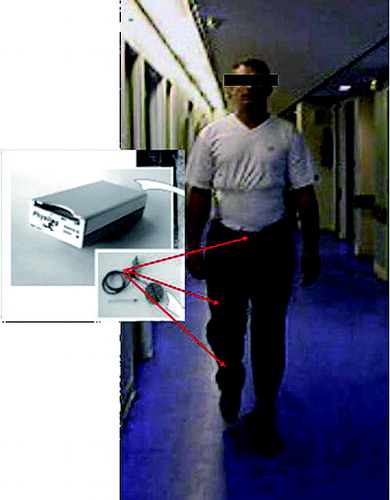
Table 1. Epidemiologic characteristics of the three groups
Table 2. The clinical scores in the groups before surgery and at 1 year follow up: Harris hip score (HHS), Postel Merle d’Aubigné (PMA), WOMAC, HOOS. Values are mean [SD] and (range)
Table 3. Femoral offset alteration in the three groups
Figure 2. Difference in knee range of motion and maximal swing speed between the operated side and the healthy limb. In contrast to the 2 other groups, in the “decreased” group there was a statistically significant decrease in the knee range of motion and the maximal swing speed during the gait cycle.
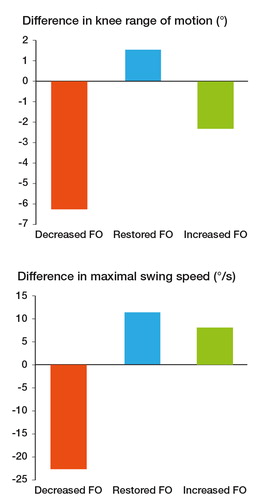
Figure 3. Passive range of motion in the 3 groups. Compared to the “restored” FO group, there was a significant decrease in adduction mobility in the “decreased” FO group.
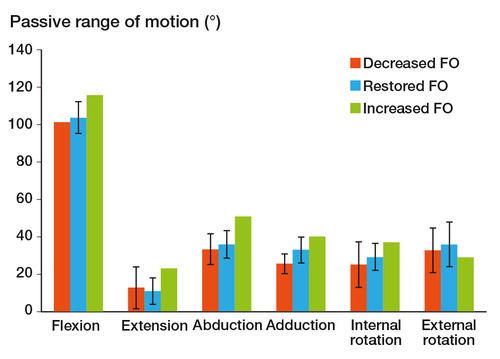
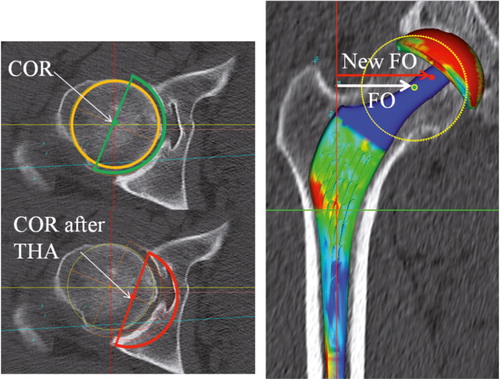
Figure 4. In some cases of dysplastic acetabula, the center of rotation has to be shifted medially. The FO may be increased in order to compensate for the decrease in acetabular offset and to avoid instability.