Figures & data
Figure 1. The diagram of repair model for each group. (A) in situ graft repair; (B) sural nerve graft by adventitial suture; (C) sural nerve graft by an adventitial suture at the proximal anastomosis and a small gap sleeve suture at the distal anastomosis, with a gap of 2 mm. CPN: the common peroneal nerve; SN: sural nerve.
Figure 2. The PFI values for each group at postoperative month 3. The sleeve suture group was superior to the adventitial suture group (P < 0.01) (n = 8). Group A: the in situ graft group; Group B: the adventitial suture group; Group C: the sleeve suture group.
Figure 3. Observation of the newly regenerated nerve in each group by the naked eye. The transplanted nerve grew well in each group, and a thickening was observed. Many newly generated tissues appear in the surrounding area. The diameter observed by the naked eye achieved or even exceeded that of the normal peroneal nerve; however, hyperplasia at the anastomoses was more obvious (black arrows). It can be seen that the chitin tube at the distal anastomosis of group C has not been fully absorbed, and the newly generated nerve tissue through the sleeve bridging technique can be observed (white arrow). (A) the in situ graft group; (B) the adventitial suture group; (C) the sleeve suture group.
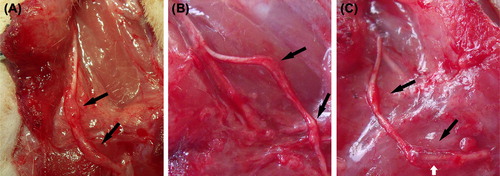
Figure 4. The motor nerve conduction velocity for the normal common peroneal nerve and for each group at postoperative month 3. There was no difference between the sleeve suture group and the adventitial suture group (n = 8). MCV: motor nerve conduction velocity; N: the normal peroneal nerve; Group A: the in situ graft group; Group B: the adventitial suture group; Group C: the sleeve suture group.
Figure 5. The degree of tetanic contraction force recovery of the tibialis anterior muscle in each group at postoperative month 3. The values for the adventitial suture group were lower than the sleeve suture group (P < 0.05) (n = 8). Recovery degree: the recovery degree of tetanic contraction force in the tibialis anterior muscle = muscle force on the right side/muscle force on the left side × 100%. Group A: the in situ graft group; Group B: the adventitial suture group; Group C: the sleeve suture group.
Table I. The maximum tetanic contraction force of the bilateral tibialis anterior muscles in each group (Newton).
Figure 6. The regeneration ratio of the regenerated nerve crossing through the distal anastomosis in each group at postoperative month 3. The values for the sleeve suture group were significantly higher than those for the adventitial suture group (P < 0.01). Regeneration ratio = the number of nerve fibers in the distal anastomosis/the number of nerve fibers in the transplanted segment (n = 8). Group A: the in situ graft group; Group B: the adventitial suture group; Group C: the sleeve suture group.
Table II. The number of nerve fibers for the regenerated nerve in each group and the normal nerve.
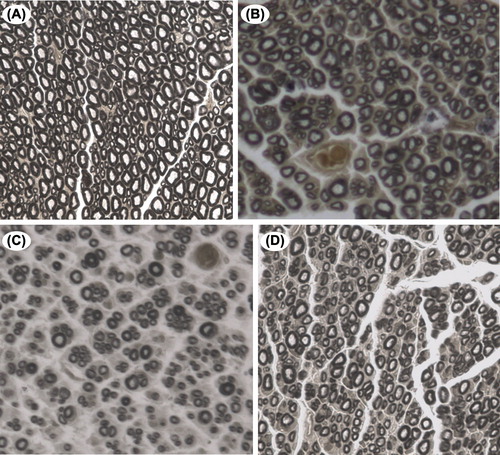
Figure 7. The osmium tetroxide staining for the distal anastomosis of the common peroneal nerve in the normal control and the experimental groups. Microscopic observation under high magnification revealed that the regenerated nerve fibers in each group had a lower degree of uniformity in the diameter compared with the normal nerve. Additionally, they were disorganized, and connective tissue was generated in the axon. The thickness of the myelin sheath of the regenerated nerve fiber was uneven, and necrosis of myelin remnants was occasionally visible (osmium tetroxide staining, 400 ×). (A) normal peroneal nerve; (B) the in situ graft group; (C) the adventitial suture group; (D) the sleeve suture group.