Abstract
In order to provide high quality services in reproductive health, training of health professionals is essential. In Turkey, a project for in-service training of medical residents was conducted in 2003 under the aegis of the Human Resources Development Foundation, the Turkish Ministry of Health and UNFPA. The project included a needs assessment, training programme development and evaluation activities. A seven-day course was developed to train institutional trainers in both training skills and reproductive health information. Fourteen experienced master trainers conducted four courses for 67 institutional trainers from 37 hospital departments in four cities, who in turn conducted a three-day programme on reproductive health topics in their respective institutions, using interactive teaching methods. 163 residents from departments of obstetrics and gynaecology, family medicine, urology, public health and paediatrics participated. Over three-quarters of trainers and residents who participated in the programme approved of the content of the courses. A limited number of topics, e.g. sexual health and adolescent reproductive health, were thought to need more attention. Trainers cited improvements in doctor–patient communication and quality of outpatient and in-patient care, and initiation of counselling in their institutions. We conclude that this training programme, attended by trainers and participants from different disciplines and using interactive teaching methods, has been successful as an effective training model for medical residents. The establishment of an ongoing collaboration between the Ministry of Health and other institutions involved in resident training in Turkey is needed to ensure the expansion of this programme to all residents in training.
Résumé
La formation est essentielle pour assurer des services de santé génésique de qualité. En Turquie, un projet de formation en cours d'emploi de résidents médicaux a été mené en 2003 sous l'égide de la Fondation pour le développement des ressources humaines, le Ministère turc de la santé et le FNUAP. Le projet comprenait une appréciation des besoins, la conception du programme de formation et des activités d'évaluation. Un cours de sept jours a été préparé pour doter des formateurs institutionnels de compétences de formation et d'information en santé génésique. Quatorze formateurs expérimentés ont mené quatre cours pour 67 formateurs institutionnels de 37 départements hospitaliers dans quatre villes, qui ont à leur tour assuré un programme de trois jours sur des thèmes de santé génésique dans leurs institutions respectives, à l'aide de méthodes interactives. Cent soixante-trois résidents de départements d'obstétrique et de gynécologie, de médecine familiale, d'urologie, de santé publique et de pédiatrie y ont participé. Plus des trois quarts des'formateurs et des résidents ayant suivi le programme ont approuvé le contenu des cours. Un nombre limité de sujets, par exemple la santé sexuelle et la santé génésique des adolescents, aurait mérité davantage d'attention aux yeux de certains. Les formateurs ont cité des améliorations dans la communication entre médecin et patient et la qualité des soins des patients hospitalisés et ambulatoires, et le lancement de services de consultation dans leurs institutions. Il est nécessaire d'établir une collaboration permanente entre le Ministère de la santé et d'autres institutions participant à la formation des résidents en Turquie pour garantir l'élargissement de ce programme à tous les résidents en formation.
Resumen
A fin de prestar servicios de salud reproductiva de alta calidad, es esencial capacitar a los profesionales de la salud. En Turquı́a, bajo la protección de la Fundación para el Desarrollo de Recursos Humanos, el Ministerio de Salud de Turquı́a y el UNFPA, se llevó a cabo en el año 2003 un proyecto de capacitación en servicio de los médicos residentes. El proyecto comprendió una evaluación de necesidades, la elaboración de un programa de capacitación y actividades de evaluación. Se creó un curso de siete dı́as para capacitar a los capacitadores institucionales tanto en las habilidades de capacitación como en la información sobre la salud reproductiva. Catorce capacitadores maestros dictaron cuatro cursos a 67 capacitadores institucionales de 37 departamentos hospitalarios en cuatro ciudades, quienes a su vez llevaron a cabo un programa de tres dı́as sobre temas de salud reproductiva en sus respectivas instituciones, usando métodos didácticos interactivos. Participaron 163 médicos residentes provenientes de departamentos de ginecologı́a y obstetricia, medicina familiar, urologı́a, salud pública y pediatrı́a. Más de tres cuartas partes de los capacitadores y médicos residentes que participaron en el programa aprobaron el contenido de los cursos. Se determinó que es necesario prestarle más atención a un número limitado de temas, p. ej., la salud sexual y la salud reproductiva de la adolescencia. Los capacitadores refirieron progreso en la comunicación médico-paciente y en la calidad de los servicios ambulatorios y hospitalarios, ası́ como el inicio de sesiones de consejerı́a en sus instituciones. A fin de garantizar la ampliación de este programa a todos los médicos residentes en formación, es esencial establecer una colaboración continua entre el Ministerio de Salud y las demás instituciones que participaron en la capacitación de los médicos residentes en Turquı́a.
Despite the marked socio-economic changes which have taken place in Turkey over the past decades, the level of reproductive and child health service provision has lagged behind, as reflected by figures on health indicators such as infant mortality (43 per 1000 live births), under-five mortality (52 per 1000 live births) and maternal mortality (estimated at 49 per 100,000 live births) rates. While almost all women in Turkey have some knowledge of at least one method of contraception, only 38% of married women of reproductive age are presently using modern methods, which is only a small increase over the 1993 rate (35%).Citation1 Citation2 One-third of mothers do not receive any antenatal care. Despite the fact that the majority (73%) of deliveries take place in a health facility and about 80% of deliveries are attended by a physician or professional midwife, maternal mortality remains high.Citation1
In Turkey, other than university hospitals, which see a relatively small portion of the population, there are two different state agencies responsible for provision of health care, namely, the Ministry of Health (MoH) and the Social Security Institution (SSK). The MoH provides reproductive health services free to the public through its network of primary health care clinics. The SSK provides health care for employees including all workers and their dependants through its own network of clinics.Citation3 Public health services offered by both MoH and SSK are often overloaded, as their resources are limited and there are problems with the quality of care they offer. The infrastructure of most public hospitals is not adequate for the provision of reproductive health services of desirable quality.Citation4 For these reasons, an increasing proportion of the population dwelling in cities are using the private sector for reproductive health care.Citation5 Particularly in private hospitals there is a focus on curative services and the specialists prefer to offer high-tech medical procedures such as in vitro fertilisation and cancer treatment, while simple but important services such as counselling and provision of educational materials are often neglected.Citation4 However, a large number of specialists are employed by the MoH and SSK on a part-time basis; thus, many of these physicians also work in private hospitals. In this context, any improvement in medical residency training programmes would reflect on the quality of services in the private sector as well.
As indicated in the International Conference on Population and Development (ICPD) Programme of Action,Citation6 Citation7 most health institutions generally lack a comprehensive approach and provision of reproductive health care is limited to counselling and services for family planning. At present there is a national effort in Turkey to improve this situation through programmes which aim to establish a comprehensive reproductive health approach in all health services including an awareness of topics such as reproductive and sexual rights, gender, adolescence, population, development and counselling.Citation8
In recent years, several projects in the area of pre- and in-service training of service providers in reproductive health have been conducted in Turkey.Citation9 Citation10 These projects have focused on general practitioners and midwives/nurses from different institutions, but have not included medical residents. In Turkey, completion of a medical residency programme of four years, which includes practical training in hospitals and outpatient clinics, is required for specialisation in clinical branches of medicine. According to MoH figures for the year 2001, the number of residentsFootnote* currently training in various branches of medicine, including obstetrics and gynaecology, family medicine, urology, public health and paediatrics, is approximately 1,800.Citation11 In addition to universities, the MoH and SSK are authorised to offer residency training programmes in their accredited teaching hospitals. Sixty per cent of the residents receive their specialisation training in teaching hospitals in the four large cities in Turkey, namely Istanbul, Ankara, Izmir and Adana. At present there are 34 teaching hospitals in these four cities, 17 of which are MoH, 9 SSK, and 8 university hospitals. The remaining residents receive their training in university hospitals situated in 33 cities around the country.
In Turkey, medical residents constitute the group which carries the major burden of health service provision in hospitals. Although medical residents work under the supervision of specialists in the field, it is usually the residents in specialities such as obstetrics and gynaecology and urology who are responsible for provision of reproductive health care, including antenatal care, delivery, treatment of sexually transmitted infections, and problems related to infertility and menopause.Citation11 Thus, it is important that medical residents are well equipped with knowledge and skills in these areas.
Taking into account this background information and aiming to contribute to the establishment of integrated and quality reproductive health services and adolescent reproductive health services, the MoH and UNFPA, following extensive consultations with Turkish academicians, have developed a reproductive health sub-programme for TurkeyCitation8 which has been expanded to contribute to in-service training of residents in reproductive health.
In this context, a project entitled “Strengthening the Quality of Reproductive Health Services through In-Service Training of Residents”, to be conducted in co-operation with the MoH, was designed and submitted to UNFPA by the Human Resources Development Foundation (HRDF), a non-governmental organisation which has carried responsibility for several reproductive health projects in Turkey.Citation9 The project aimed to achieve four complementary goals, namely: 1) to assess residents' training needs on reproductive health, 2) to prepare and conduct a trial training programme for residents, 3) to evaluate the trial training programme activities, and 4) to strengthen the training activities in this context.
As the implementing agency of the project, HRDF was responsible for the overall co-ordination of these activities and asked the Woman and Child Health Training and Research Unit and the Department of Public Health of the Istanbul Faculty of Medicine to take part in the project. Our tasks were to: 1) conduct a situation analysis for assessment of needs, 2) develop the training programme and 3) undertake the evaluation of the trial phase. Our experiences in carrying out the work in these three areas are described in this paper.
Methodology
For reasons of ease of accessibility, more suitable facilities and existing potential for better use of resources, 34 teaching hospitals situated in Istanbul, Ankara, Izmir and Adana, where most residents are currently being trained, were selected for the initial phase of the project. These hospitals included residents in 135 departments of obstetrics and gynaecology, family medicine, urology, public health and paediatrics in the 34 hospitals. A military teaching hospital was subsequently added to this list upon their request.
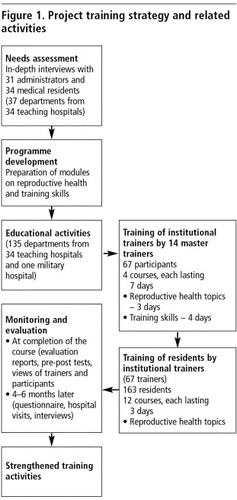
A flow chart summarising the project strategy and related activities directed at this group is presented in .
Figure 1 Project training strategy and related activities.
Assessment of needs
This initial phase of the project focused on assessment of the residents with regard to their educational needs in the area of reproductive health. This assessment constituted the background for the formulation of an educational programme to meet those needs. The data for the assessment were collected by visiting the selected teaching hospitals and by conducting in-depth interviews with one administrator and one resident from each of the 37 participating departments of the hospital. Thirty-one administrators and 34 residents could be reached and interviewed in depth. Two members of the team conducted these semi-structured interviews, which consisted of questions on the current training programme and on the health service provision offered by the institution. Given the definition of reproductive health introduced by ICPD, interviewees were asked questions such as whether basic services should be provided according to this definition, which basic services were offered by their institution, their views on how to improve services according to the needs of the patients, and what kind of education and training in these subjects they had received as opposed to what they needed.
Figure 2 Citrus conditioning plant, Turkey. 2002
The results of these in-depth interviews revealed that educational activities for the residents including seminars, journal club, statistical evaluation, case discussion meetings, bedside (or practical) teaching and intra- or inter-departmental rotations were currently being conducted in almost all of the clinics. However, the focus of the training programmes was very much influenced by the areas of interest of the clinic directors involved. The findings, which were quite similar for all hospital departments, showed that the residents had indeed received some information on reproductive health that was relevant to their speciality, but that a uniform and comprehensive approach was lacking. For example, residents training in obstetrics and gynaecology stated that they had been provided with adequate information on subjects such as antenatal care, delivery, contraception and sexually transmitted infections, but that they were not being trained to be proficient in IUD insertion, diaphragm fitting and condom promotion, or in counselling skills. Paediatric residents from most of the hospitals stated that their training programme did not cover reproductive health and that they were unable to provide information to parents on these issues. The responses enabled us to identify the basic educational needs, which included sexual health, adolescent services, infection prevention and quality of services. Some examples of other opinions expressed during the needs assessment were that the training programmes would be enhanced by including educators and participants from different disciplines, and by application of participatory teaching techniqes in the training.
Development of the training-of-trainers programme
The next step in the project was to train the individuals who would act as institutional trainers by improving their training skills and strengthening their knowledge of reproductive health. The main criteria for the selection of institutional trainers were academic performance and volunteering for the task. Care was taken to have trainers who belonged to the different medical specialities as well. Master trainers, individuals who would be responsible for the training of the institutional trainers, consisted of 14 individuals who had previously trained and worked as trainers in national MoH projects on reproductive health, from the disciplines of health education (1), public health (5), family medicine (2), general practice (2), obstetrics and gynaecology (1), urology (1), paediatrics (1) and psychiatry (1). The courses were designed to be multidisciplinary. The institutional trainers would attend the training-of-trainers courses in groups and the sharing of experiences would serve as a tool to acquire a wider outlook on the meaning of comprehensive care. To this end, a seven-day training programme with four days allotted for training skills and three days for acquisition of information on reproductive health was planned. The reproductive health section of the programme also constituted the basis of the three-day course offered to the residents in the next phase.
The objectives of the reproductive health section of the programme were to provide:
basic information about the state of reproductive health in the world and in Turkey (demographic changes, population policies and regulation)
basic concepts about reproductive heath (ICPD Programme of Action, definitions and a comprehensive care approach)
the importance of sexual health, of a satisfying and safe sexual life (definitions, sexual identity, value classification, sexuality in society, safer sex)
the characteristics of high quality services in reproductive health (choice, information given, interpersonal relations, patients' rights, technical competency, follow-up and continuityCitation12)
the principles of fertility regulation and counselling (impact on maternal and child health, contraception, eligibility criteria and counselling)
the process leading to safe motherhood, safe reproductive health and healthy children (antenatal and delivery services, post-partum care, abortion and post-abortion care)
reproductive health in adolescence and the sexual education needs of adolescents (puberty, sexual education)
the basic principles of infection prevention in reproductive health care (decontamination, disinfecting, sterilisation of equipment and handling of waste products)
the importance of diagnosis and treatment of sexually transmitted infections and other genital tract infections (prevention, case management)
the principles of early diagnosis of frequently seen cancers in reproductive organs (cervix, breast, prostate, testes).
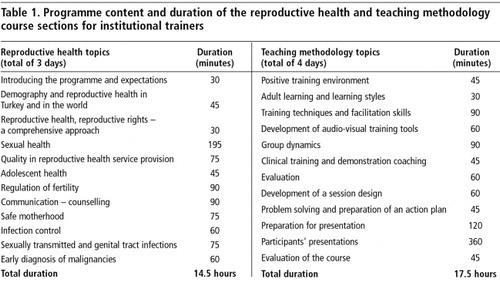
The objectives of the training skills section of the programme were formulated based on previous experience at the Istanbul Faculty of Medicine.Citation13 A summary of the programme content and duration of the course offered to the institutional trainers is given in Table 1.
The next step was for the master trainers to prepare teaching modules for each of the topics listed in Table 1, in accordance with the course objectives.
Educational activities
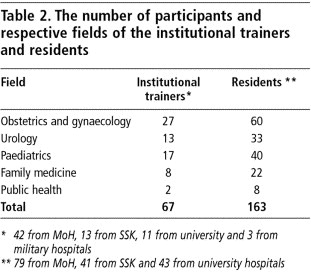
The master trainers trained a total of 67 institutional trainers working in different institutions. Four seven-day courses were held in different locations, two in Istanbul, the others in Ankara and Izmir. The 67 institutional trainers who completed the course conducted the training programmes on reproductive health for 163 residents in their respective institutions. The fields of speciality of the institutional trainers and residents who received the training are shown(Table 2).
The training of 163 residents by the 67 institutional trainers was realised by conducting 12 courses on reproductive health, each lasting three days, between December 2002 and February 2003. Completion of a minimum of two years' training and volunteering for the training constituted the criteria for selection of the residents. The number of institutional trainers conducting these courses varied between two and nine trainers per course. One master trainer was also present at each course to supply feedback to the institutional trainers and to act as a supervisor. Groups of residents from different disciplines, and at times, residents working in different institutions attended these courses (Table 2). Nine of the 12 courses were held in suitable sites outside the hospitals and the other three in the hospitals.
The training methods employed in all courses were completely based on participatory techniques such as small group discussions, role-playing, case study, brainstorming and experience-based learning.
Evaluation
Assessment of the educational activities was limited to the views expressed by the trainers and residents. Evaluation tools used at the completion of the courses were:
progress reports written by the master trainers
forms filled out by the institutional trainers for assessment of the course and for their self-assessment
forms for assessment of the course filled out by the residents
pre- and post-tests scores of the institutional trainers and the residents
master trainers' reports on courses conducted by the institutional trainers.
Four to six months after completion of the courses, the participants were asked for an evaluation of the impact of the educational process which they had been through. This information was collected through a written, open-ended questionnaire designed for this purpose and mailed to all participants. The questionnaire included questions on their views on the content and duration of the course, the impact of the course on service provision in their institution and what they thought about the future expansion of these courses.
In addition, after 6–9 months, site visits were made to four institutions (two MoH and two SSK hospitals) and interviews were held with the institutional trainers, the residents who had been on the courses and the administrators in one group. The visiting team consisted of two of the members of the research team and one representative each from the MoH and SKK. The interviews aimed to determine whether the hospital administrations were aware of these educational activities, to obtain their views on the impact of the courses on service provision in reproductive health in their respective institutions and whether they thought these activities should be continued. In fact, in general the administrators were not fully aware of the project. Only those who were responsible for the co-ordination of the educational activities within the hospital had some idea that a course had been conducted, but even these administrators were not aware of the course content. These findings indicated that although the institutional trainers spent a lot of time and effort on conducting the courses, they had not been sufficiently active in establishing the right kind of communication and advocacy within their institutions.
Evaluation of the courses for institutional trainers
The tests given at the completion of the courses showed that at least 80% of the institutional trainers were able to give correct answers to questions covering all sessions. The most significant increase in scores occurred with the topic on quality in health service provision. The lowest scores were on sexual health, which indicated that this module needed to be reviewed.
The overall opinions of the master trainers were mostly positive; they thought the courses had attained their objectives and had served to increase the level of motivation of the participants. Some negative points raised were the inability to reach the desired standard in some of the courses and a lack of awareness of some of the participants of the objectives and content of the course. This lack of awareness was attributed to failure to provide adequate information beforehand by the institutional authorities.
The institutional trainers thought that the courses were satisfactory both in content and in presentation overall. The mean score for content was 4.68 (out of 5). The negative comments were centred on two main points, namely, that some participants were asked to attend the course without prior knowledge of its purpose and content, and without being asked if they were willing to participate. In fact, the proportion of participants who attended the courses willingly was 57%.
Evaluation of the courses for the residents
At the completion of the courses for the residents, their overall scores increased significantly and at least 87% gave correct answers.
The views expressed by the institutional trainers were positive. They thought that the courses had attained their objectives and that most of the residents had attended the courses willingly. They thought continuation of this type of educational effort was important and would bring about the desired changes in attitude. They also believed in the advantages of recruiting trainers on a volunteer basis.
The residents also thought that the courses had attained their objective. The mean score given for content was 4.48 (out of 5). They thought that the courses should preferably be held outside the hospital and that the presence of all trainers throughout the duration of the course would improve the outcomes. Most residents thought the courses should be attended by all residents, all practitioners, all heads of section and all teaching staff. Only a few participants labelled it a waste of time and money. The majority (73%) of the residents said they had attended the course voluntarily, but fewer (40%) had been informed about the objectives or content of the course beforehand. A number of the residents pointed to the absence in the programme of topics such as infertility, menopause, management of sexual problems, sexual abuse, psychological development, screening tests, breastfeeding and immunisation of infants. Two-thirds of the residents said they had now become aware of their responsibilities in this area. The other third had no comments on this question.
The most frequent comments made by the master trainers and the institutional trainers in their evaluation sessions were that the courses had been productive, that the atmosphere had been motivating and at the same time friendly, that they had acquired new concepts and that the training had been effective.
Evaluation four to six months after completion of the courses
An evaluation of the project four to six months after the end of the courses was done using a questionnaire sent to the trainers and to the residents. All the master trainers, 85% of the institutional trainers and 62% of the residents responded.
All the institutional trainers said they were presently using the teaching techniques they had learned. The majority were now encouraging their patients to ask questions, using the communication skills they had learned and formulating their objectives and purposes prior to the educational session. They cited improvements in doctor-patient communication, improvements in quality of out-patient services, initiation of counselling services and improvements in quality of in-patient care in their institutions. These responses were indeed exciting in that they show it may be possible to bring about changes in service provision in these particular health institutions through the training of individuals, without the need for administrative reforms.
When asked whether attendance at the three-day course had affected their subsequent performance, 21 of the 101 residents who responded stated that the quality of their service provision in the out-patient clinic had improved, 14 saw improvement in their in-patient service provision, 27 improvement in their communication with their patients and 16 that they had started offering counselling services. All the trainers and residents stated that the multidisciplinary nature of the participation was of great help to them in understanding the meaning of a comprehensive approach to reproductive health. Below are some examples of views on this issue:
“This course made me aware of health subjects outside of my speciality. I now believe in the need for a multidisciplinary approach in health care.”
“In this course I acquired valuable information on subjects within my own medical specialty as well as in other specialties involved in reproductive health. I have also gained a new approach on how to convey this information to the public.”
“I was only paying attention to the child and was not providing the parents with any information on contraception. Now I know that I should also address the parents.”
As regards content and duration of each session of the reproductive health component of the course, the master trainers thought that the session on regulation of fertility was too short. All trainers and residents agreed that the content of the session on sexual health was not satisfactory and did not adequately address topics such as approach to sexual problems or disorders in sexual function. They also felt that the time allotted to the session on adolescent health was inadequate and should be lengthened to include topics such as adolescent psychology and sexual abuse.
Overall, with these exceptions, both duration and content of each module of the courses was scored high by 80–100% of master trainers, institutional trainers and residents, and the content of the three-day course offered to the residents was found to be satisfactory (data not shown).
“What is important is to provide a frame and show the way to explore the sources of information. The main objective of the course will be lost if the programme is loaded with too many details.” (Master trainer)
According to the master trainers, in order to assure continuity, the course objectives need to be included in the logbook recordsFootnote* kept by residents, and training in reproductive health needs to be included in the standard programme for resident training. Similar suggestions were made by the institutional trainers and the residents. It was suggested that professional physicians' associations could be a possible source of support for these activities.
Discussion
The findings of this educational intervention indicate that the three-day training programme on reproductive health topics was quite adequate in meeting the need for information. Over three-quarters of the master trainers, institutional trainers and residents who participated in the programme approved of the content and duration of the courses. A limited number of topics, i.e. sexual health and reproductive health in adolescence, were thought to need revision or additions. Indeed, as regards the topic of sexual health, because the master trainers were not experienced on the issue, we have encountered difficulties in integrating information on this topic into the course programme. Experts in this field are indeed scarce in Turkey and we believe that in future programmes they should take part in the preparation and implementation of the modules relating to this topic.
As to the residents' request for inclusion of additional topics, the programme for these courses was designed to address residents in five different specialities and therefore, to cover only the basic topics of reproductive health. Moreover, the programme content was based on an assessment of the residents' needs. We believe it will be more realistic to cover the more specialised topics in the routine training programmes of each speciality rather than expand this programme. Prolonging the duration of the courses may also create difficulties in implementation.
Klufio et al have stated that a time period of at least 8 to 10 years is needed for educational programmes to have a lasting impact on quality of health service provision and to reflect on health indicators.Citation14 For this reason, evaluation of acquisition of knowledge is accepted as the first step in monitoring the efficacy of a new training programme. At the completion of the project it will be possible to make a more general evaluation, since the evaluation will also include the views of the recipients of reproductive health services. Some changes in health indicators may also become apparent at the end of 8–10 years and these may be used in the evaluation.
Various studies have shown that educational exercises conducted using interactive teaching methods are more productive in bringing about changes in attitude and also in having a more lasting impact.Citation13 Citation15 Citation16 Interactive teaching has been shown to be particularly effective in educational programmes in the area of reproductive health,Citation9 and the participants in this project found it instructive and useful.
A holistic approach to reproductive health entails co-operation and sharing of responsibilities between various medical specialities. This approach serves to minimalise missed opportunities as well as to encourage improvements in quality of service provision. The contribution of an interdisciplinary approach to women's health has been shown in a recent interdisciplinary study conducted by a Yale University team,Citation17 and participants of the present project shared this view. Multidisciplinary attendance is necessary for an interactive training environment and will also be effective in establishing collaboration and synergy among various specialities and among service providers working in different institutions.
In light of the findings of this study, we believe that to attain a comprehensive approach, it is important to integrate training in reproductive health within the existing residency training programmes in Turkey. The courses on reproductive health can be conducted separately, by allotting three days to the subject without expanding the content too much. We also believe it is essential that attendance be multidisciplinary and that the trainers be from a multidisciplinary background. Volunteering for the task should also be considered an important aspect in the selection of institutional trainers and residents. In addition, administrative support and advocacy in hospitals are important elements in initiating a comprehensive approach to reproductive health services. Although the attitudes of some trainers in subjects such as obstetrics and gynaecology may be expected to be conservative and difficult to change,Citation18 meetings at the local level to which administrators are also invited along with individuals who will act as the co-ordinators will enhance communication and may be helpful in establishing the desired objectives.
To be able to expand these educational programmes to all residents in training around the country and to ensure their continuity, special protocols need to be developed for various institutions involved with training of medical residents, such as the MoH, SSK and Council for Higher Education. The Human Resource Development Foundation is trying to facilitate this process. There is also a need for dissemination of information to the relevant institutions and hospitals, and to trainers, on the need for information in the area of sexual and reproductive health as well as on the educational activities that have taken place to date. A periodical entitled “Bulletin for Reproductive Health” and e-mail groups may be of help in the dissemination of information and will also help to establish communication among residents in various disciplines.
Acknowledgements
We wish to express our thanks to all trainers and participants in this project for answering the questionnaire and giving valuable comments on the courses. We wish also to thank Dr Demet Gural and her colleagues from the Human Resource Development Foundation for their contributions to the planning and conduct of the project. This work was supported by the UNFPA 3rd Country Programme for Turkey (Project Number TUR/03/01/06-01/P06) and conducted by the Human Resource Development Foundation in co-operation with the Ministry of Health, Turkey.
Notes
* In Turkey, residents are physicians who are in the process of getting specialist training.
* A booklet listing the core information and skills that the residents need to acquire during their training.
References
- Turkish Demographic and Health Survey, 1998. 1998; Ministry of Health, Hacettepe University, Institute of Population Studies and Macro International: Ankara.
- Turkish Demographic and Health Survey, 1993. 1993; Ministry of Health, Hacettepe University, Institute of Population Studies and Macro International: Ankara.
- SB Savas, O Karahan, O Saka. Health care systems in transition, Turkey. Copenhagen European Observatory on Health Care Systems. 4(4): 2002; 71–77.
- Management Sciences for Health. Research on Quality in Family Planning, Istanbul, Adana, Içel, 1998–2001. 2002; Ministry of Health, Maternal and Child Health/Family Planning Directorate Publications: Ankara.
- World Bank Report 2003. Turkey: Reforming the Health Sector for Improved Access and Efficiency. Human Development Sector Unit, Europe and Central Asia Region. Report No. 24358-TU. 2003; World Bank: Washington DC.
- United Nations. Programme of Action, adopted at the International Conference on Population and Development, Cairo, 5–13 September 1994.
- United Nations. Key Actions for the Further Implementation of the Programme of Action of the International Conference on Population and Development adopted at the twenty-first special session of the General Assembly, New York, 30 June–2 July 1999.
- Sub-Programme Document between the Government of Turkey and the United Nations Population Fund, Ankara, January 2001.
- SB Ozvaris, BO Oncuer, M Bertan. A new model for education in medical schools. Presented at Symposium on Continuous Quality Control in University Education, Ankara, May, 1997. Symposium Abstract Book. 1997; 275–286.
- SB Ozvaris, BO Oncuer, M Bertan. A new approach for strengthening of undergraduate family planning training in medical faculties. Bulletin of Hacettepe Community Medicine. 1: 1996; 1–4.
- Strengthening the quality of reproductive health services through in-service training of residents. TUR/03/01/06-01/P06. Ankara, 2001. Unpublished Project Document.
- J Bruce. Fundamental elements of the quality of care: a simple framework. Studies in Family Planning. 21(2): 1990; 61–91.
- N Yolsal, A Bulut, S Karabey. Development of training of trainers programmes and evaluation of their effectiveness in Istanbul, Turkey. Medical Teacher. 25(3): 2003; 319–324.
- CA Klufio, EY Kwawukume, KA Danso. Ghana postgraduate obstetrics/gynecology collaborative residency training program: success story and model for Africa. American Journal of Obstetrics and Gynecology. 18932003; 692–696.
- Y Steinert, LS Snell. Interactive lecturing: strategies for increasing participation in large group presentations. Medical Teacher. 21(1): 1999; 37–42.
- LB Weiss, SP Levison. Tools for integrating women's health into medical education: clinical cases and concept mapping. Academic Medicine. 75: 2002; 1081–1086.
- JB Henrich, JT Chambers, JL Steiner. Development of an interdisciplinary women's health training model. Academic Medicine. 78(9): 2003; 877–884.
- M Haslegrave, O Olatunbosun. Incorporating sexual and reproductive health care in the medical curriculum in developing countries. Reproductive Health Matters. 11(21): 2003; 49–58.