
Abstract
Objective: To explore caries development in children from 5 to 12 years of age, and to study whether enamel caries and dentine caries at 5 years of age could predict caries prevalence at 12 years of age, controlled for child characteristics.
Methods: The study included 3282 children examined at 5 and 12 years of age. Data were collected by clinical examination and questionnaire. Enamel and dentine caries were registered at surface level. Data were tested by t-test and analysed by bi- and multivariate logistic regression. The study was ethically approved.
Results: In 5-year-olds, 15% of the children had dentine caries experience and 21% had enamel caries. In 12-year-olds, 32% had dentine caries experience and 47% had enamel caries. Children with dentine caries experience at 5 years of age had at 12 years of age developed more surfaces with enamel caries (mean 2.8, SD 4.2) and dentine caries experience (mean 1.8, SD 2.5) than other children (p < .05). Dentine caries experience at 12 years of age was associated with having only enamel caries (OR 1.6, CI 1.2–2.0) and dentine caries experience (OR 3.2, CI 2.6–3.9) at 5 years of age. Family status and parental education were related to caries development.
Conclusion: Children with caries in primary teeth continued to be caries risk children during the mixed dentition period. In addition to dentine caries experience, enamel caries in primary teeth was a predictor for caries development in young permanent teeth and may be used to improve the caries risk assessment.
Introduction
Caries prevalence in Western countries has declined in recent decades, but caries is still a common disease in children [Citation1–3]. The distribution is skewed, and the majority of children have no caries, while some have many decayed teeth and require extensive dental care [Citation2–4]. Caries prevalence has been reported to increase during childhood from primary to permanent dentition [Citation3]. In Europe, 20% to 55% of 5-year-olds and 30% to 70% of 12-year-olds have been described to have dentine caries experience [Citation3–8].
Longitudinal studies may increase understanding of caries development in children. Few longitudinal studies have been performed on caries development in the period permanent teeth erupt [Citation6,Citation9–11]. Most of these studies have limitations, such as few participants, and have been conducted in selected groups, or they have not included socio-economic conditions or enamel caries [Citation9–11]. Knowledge concerning longitudinal development of enamel and dentine caries at individual level in children during the period of mixed dentition is scarce [Citation12].
To initiate preventive measures and reduce caries development, caries risk in children has to be identified. It has been reported that dentine caries in primary teeth has been a useful predictor for caries development in permanent teeth [Citation9–11,Citation13]. Because of the increasing proportion of 5-year-olds being dentine caries free, other predictors may be considered, such as clinical findings at dental examinations, enamel caries, oral health behaviour or socio-economic conditions of the family. In preschool children, socio-economic conditions of the family have been associated with caries development. Children having parents with low education, non-Western background or lacking parental guidance regarding oral health have been reported to have higher caries prevalence in primary teeth than other children [Citation14–18], while few studies have evaluated associations between caries development from 5 to 12 years of age and family status [Citation19]. To our knowledge, no studies have used enamel caries in primary teeth as predictor for caries development in permanent teeth.
In Norway, all children are entitled to dental care free of charge in the public dental service from birth to 18 years of age. This gives opportunity to monitor a large group of children and study the longitudinal development of enamel and dentine caries. They are called for examination at individual intervals and offered all dental care deemed necessary, both non-operative and operative treatments. All children are recommended to brush twice daily with fluoridated toothpaste from eruption of the first tooth. Individual preventive treatment is provided based on dental professionals’ judgement of each patients’ need and may include sealants, fluoride varnish, instruction and motivation on oral health behaviour (oral hygiene and sugar consumption), as taught at the universities and recommended in the dental services in Norway during the last 20 years. Drinking water is not fluoridated, and fluoride level is low.
In this prospective longitudinal study, the overall objective was to explore caries development in children from 5 to 12 years of age. The specific objectives were to describe caries status at both ages and to study whether enamel caries and dentine caries at 5 years of age could be used as predictors for caries prevalence at 12 years of age, controlled for child characteristics.
Materials and method
Study population
All children born in 2002 (n = 7002) in one county (Akershus) were in 2007 invited to participate in the study at 5 years of age. The county had 600,000, fourteen percent of the Norwegian population. In total, 5623 children (80%) were included. Non-participants were either those who did not want to participate, children who did not show up and children who were not invited by the dental personnel. Mean age at examination was 5.2 years (SD 0.4). In 2014, at 12 years of age children were invited to a follow-up examination, and 3282 (58%) were available for examination. Mean age at the follow-up examination was 12.1 (SD 0.5) years. In the studied county, dentine caries prevalence was similar to the national average (20% vs 24% in 5-year-olds and 37% vs 40% in 12-year-olds) [Citation2].
Methods
Data were collected by clinical and radiographic examination at routine dental visits in children at 5 and 12 years of age. Examinations at 5 years of age were performed by 44 hygienists, and examinations at 12 years of age were performed by 45 dentists and 46 hygienists as part of the regular dental examination in the dental services. During examinations at 5 years of age, parents filled in a questionnaire with information regarding child characteristics.
At 5 years of age, caries was registered in primary teeth, and at 12 years of age, caries was registered in permanent teeth. Radiographs were taken in accordance with standard routine in dental services (when visual inspection of approximal surfaces was impossible) and used in addition to clinical caries registration in 73% of 5-year-olds and 97% of 12-year-olds. Caries experience was registered with tooth surface as unit of measurement using DMF index and reported at surface and tooth level. Five caries grades (d1–5) were recorded [Citation20]. Grade d1–2 were enamel lesions, and d3–5 were dentine lesions. Caries was categorized as only enamel caries (d1–2), and dentine caries experience with or without enamel caries (d3–5).
Intra- and interexaminer agreement
Written and oral information about the caries criteria was given to and discussed with the examiners before data collection started. The dentists and hygienists are calibrated on regular basis as part of routines in the dental services. A gold standard based on the second and third authors’ registrations was compared with the examiners’ registrations. Using Cohen’s kappa intra- and interexaminer agreements were tested based on 20 bitewing radiographs of primary molars including 8 approximal surfaces in each radiograph. Mean intra- and interexaminer values were 0.85 (SD 0.12) and 0.86 (SD 0.10). Intra- and interexaminer agreements were based on 8 radiographs of permanent molars including 12 approximal surfaces in each radiograph. The mean intra- and interexaminer values were 0.69 (SD 0.16) and 0.69 (SD 0.17). Cohen’s kappa was categorized as substantial to almost perfect agreement [Citation21].
Questionnaire
The questions provided information about child’s gender, parents’ national background, parents’ education and family situation.
Parents’ national background was registered as mother and father’s country of birth. The results were combined into one variable and dichotomized into both parents having Western background and one or both having non-Western background. Non-Western background included parents born in Asia, Africa, South America, Central America and Eastern Europe.
Education was registered as mother’s and father’s length of education, combined into one variable and dichotomized into both parents having high education and one or both parents having low education. More than 12 years at school were defined as high education, and 12 years or fewer were defined as low education.
Family status was measured as child living with mother and father; two-parent family, or living with mother or father; one-parent family at 5 years of age.
Ethical aspects
Written, informed consent was obtained from parents at both examinations. The Regional Committee for Medical Research Ethics approved the study (2.200.54 and 2013/1881).
Statistical analysis
The statistical analyses were conducted using IBM SPSS statistics, version 25 (Armonk, NY, USA). Differences in caries experience were tested with t-test. Bi- and multivariate logistic regression analysis was performed with children’s dentine caries prevalence (the presence/absence of dentine caries) at 12 years of age as dependent variable. Spearman’s rank correlation was calculated before multivariate logistics regression analysis to explore associations between the independent variables. High correlation was found between dentine caries experience and approximal dentine caries experience (Spearman’s rho = 0.8) and between enamel caries and approximal enamel caries (Spearman’s rho = 0.7) at 5 years of age. As a consequence, approximal caries was not included in multivariate analysis. Data were presented by using frequency, mean with standard deviation (SD), odds ratio (OR) with 95% confidence interval (CI) and SiC Index to describe caries status at 12 years of age. The level of significance was set at p < .05.
Results
The majority of children that participated had parents with Western background, high education and lived in two-parent families at 5 years of age ().
Table 1. Children according to gender, parental background, parental education and family status (n = 3282).
No statistical significant differences were found between children examined only at 5 years of age, and children examined at both ages regarding caries prevalence (17% vs 16%), non-western background (13% vs 12%) and low parental education (17% vs 16%). Children examined only at 5 years of age had higher mean number of teeth with caries experience (0.7 vs 0.6, p < .05) than children examined at both ages.
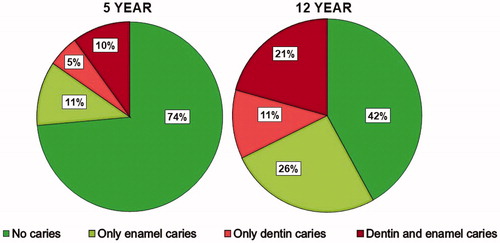
displays the children’s caries status at 5 and 12 years of age. At 5 years of age, 74% of the children had neither enamel nor dentine caries experience. Seven years later, the proportion of children with no signs of caries was reduced to 42%. Proportion of children with enamel and dentine caries experience more than doubled in the period, enamel caries from 21% to 47% and dentine caries experience from 15% to 32%.
Figure 1. Proportion of 5- and 12-year-old children according to caries status (n = 3282).
Caries status at tooth and surface level in all children and in children with dentine caries experience at 5 and 12 years of age is presented in and . Children with dentine caries experience had at 5 years of age on average 3.5 (SD 2.9) teeth with dentine caries experience and at 12 years of age 2.0 (SD 1.3) teeth with dentine caries experience. The main part of dentine caries experience at 5 years of age was decayed teeth, and at 12 years of age, the main part was filled teeth. The difference between the number of teeth and surfaces with dentine caries experience was low at both ages. The SiC Index at 12 years of age was 1.9 (SD 1.3).
Table 2. Dentine caries experience at tooth and surface level in children at 5 years of age. All children (n = 3282) and children with dentine caries experience (n = 510).
Table 3. Dentine caries experience at tooth and surface level in children at 12 years of age. All children (n = 3282) and children with dentine caries experience (n = 1060).
Approximal dentine caries experience was registered in 10% of the children at 5 years of age, and in 6% at 12 years of age. Children with approximal dentine caries experience had at 5 years of age on average 3.0 (SD 2.4), and at 12 years of age 1.5 (SD 1.1) decayed or filled approximal surfaces (results not shown).
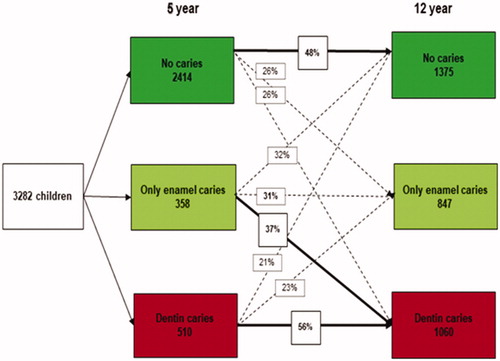
The longitudinal changes in caries prevalence in children from 5 to 12 years of age are illustrated in . Of children with no caries experience at 5 years of age, 48% still had no caries experience at 12 years of age. Of children with only enamel caries at 5 years of age, 37% developed dentine caries experience at 12 years of age. More than half of children (56%) with dentine caries experience at 5 years of age had dentine caries experience at 12 years of age.
Figure 2. Longitudinal changes in enamel and dentine caries prevalence in children from 5 to 12 years of age.
presents numbers of surfaces with enamel caries and dentine caries experience at 12 years of age according to dentine caries prevalence at 5 years of age. Children with dentine caries experience at 5 years of age had at 12 years of age developed more surfaces with enamel caries (mean 2.8, SD 4.2) and dentine caries experience (mean 1.8, SD 2.5) than children without dentine caries at 5 years of age (p < .05).
Table 4. Number of surfaces with enamel caries and dentine caries experience at 12 years of age related to dentine caries prevalence at 5 years of age, mean (SD) (n = 3282).
shows results from bi- and multivariate logistic regression analyses exploring association between caries variables at 5 years of age and dentine caries prevalence at 12 years of age, controlled for child characteristics. The results from the multivariate analysis showed that children with only enamel caries at 5 years of age had 1.6 times higher probability of developing dentine caries experience at 12 years of age than children without caries at 5 years of age. Children who had dentine caries experience at 5 years of age had 3.2 times higher probability of developing dentine caries experience at 12 years of age than other children. Living in one-parent family at 5 years of age and having parents with low education were associated with dentine caries experience at 12 years of age.
Table 5. Children with dentine caries experience at 12 years of age according to caries variables controlled for child characteristics at 5 years of age. Bivariate and multivariate logistic regression analyses.
Discussion
This longitudinal study explored caries development in children from 5 to 12 years of age and aimed to identify predictors of caries prevalence at 12 years of age. One finding was that proportion of children with enamel caries and dentine caries experience doubled during these seven years. Enamel caries and dentine caries experience at 5 years of age predicted caries development in the young permanent dentition.
In this study, proportion of children with dentine caries prevalence at 5 years of age was slightly lower than reported in international studies [Citation3,Citation5,Citation7], while proportion of children with dentine caries prevalence at 12 years of age was similar to other European studies [Citation3,Citation6–8]. The results in this study showed that children at 12 years of age had on average three surfaces with enamel caries and two teeth with dentine caries experience. This indicates that the children will require lifelong maintenance. Few surfaces were registered with approximal dentine caries experience at 12 years of age, suggesting that the majority of teeth had dentine caries experience in occlusal surfaces. The results suggest that increasing the use of sealants may have opportunity to prevent caries development in occlusal surfaces in newly erupted permanent molars. Previous findings have also shown that the occlusal surface is the most caries prone surface in the young permanent dentition [Citation7,Citation22].
Enamel caries has seldom been reported in previous studies. The results from this study revealed high prevalence of enamel caries. Having enamel caries or dentine caries experience at 5 years of age was associated with dentine caries prevalence at 12 years of age. The findings imply that both enamel caries and dentine caries experience at 5 years of age could be used as predictors for further caries development. The results suggest that recording enamel caries provides opportunity for a more accurate caries risk assessment in populations with no or low dentine caries prevalence [Citation3,Citation13,Citation20] and may increase the opportunity to prevent further caries development by using non-operative approach and avoid restoration [Citation23]. The results support earlier studies that suggest dentine caries development in primary teeth as predictor for further dentine caries development [Citation9,Citation10,Citation13].
It is documented that parental background and education are associated with preschool children’s caries development. Preschool children depend on parents’ ability to establish and maintain favourable oral health behaviour [Citation14]. An ongoing detachment and social equalization among 12-year-olds imply that peers and other adults play a more important role in children’s life and oral health as they grow older [Citation17,Citation24]. In this study, dentine caries experience at 12 years of age was associated with both parental education and family status at 5 years of age, showing that family still is important for older children’s dental health and that parents’ guidance has positive effects.
One strength of this study was the longitudinal follow-up of a large sample over 7 years. In longitudinal studies, non-participation and dropout may cause selection bias. In this study, children who dropped out had higher number of carious teeth, but the difference was small (0.1 tooth). Dropout may have resulted in underestimation of dentine caries prevalence in the studied area. Dentine caries experience, parents’ background and educational level in the studied children were similar to national average [Citation2]. It is reasonable to assume that the results were representative for the country in general. The study was based on questionnaire and clinical examination. Questionnaires may have limitations such as non-response, misconceptions and answering in a social favourable way [Citation25]. The questions in this study were considered uncomplicated, relating to child characteristics and therefore assumed to reduce recall and report errors. The clinical examinations were performed by experienced dentists and hygienists in dental clinics, and the calibration showed substantial to almost perfect agreement [Citation21].
One finding in the study was that children who had caries before 5 years of age developed more caries in the period from 5 to 12 years of age than children who were caries-free at age 5 years. This indicates that the preventive treatment provided in the period was not sufficient to establish oral habits necessary to prevent caries development in newly erupted permanent teeth. One study has shown that children who develop caries before 2 years of age had more caries at 5 years of age than children without caries at age 2 years [Citation26]. The results from this study suggest that children who develop caries soon after the eruption of primary teeth have increased caries risk also in the young permanent dentition.
An adjustment of caries risk assessment taking into account enamel caries in addition to dentine caries experience may have the potential to reduce caries development in the permanent dentition. Individual instruction and motivation for oral care should be provided towards the parent before the age of 5 years. Initiation of favourable oral health habits should preferably start when the first primary tooth erupts. In Norway, collaboration between general health services and dental services is established [Citation26,Citation27]. New national guidelines regarding oral care in children younger than 3 years of age were introduced in 2019 [Citation28,Citation29]. The guidelines increase the focus on early caries risk assessment and collaboration between the general health services and dental services to provide preventive oral health care to young children and their parents.
In conclusion, children with caries in primary teeth continued to be caries risk children during the mixed dentition period. Enamel caries and dentine caries experience in primary teeth may be used as predictors for caries development in young permanent teeth and may have lifelong consequences.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Steiner M, Menghini G, Marthaler TM, et al. Changes in dental caries in Zurich school-children over a period of 45 years. Schweiz Monatsschr Zahnmed. 2010;120(12):1084–1104.
- Statistics Norway. Dental status by age. Statistisk sentralbyrå; [cited 2020]. Available from: http://www.ssb.no/en/statbank/table/04163/tableViewLayout1/?rxid=f4253601-e8c8-4896-8836-2520e151b612
- Koch G, Helkimo AN, Ullbro C. Caries prevalence and distribution in individuals aged 3-20 years in Jönköping, Sweden: trends over 40 years. Eur Arch Paediatr Dent. 2017;18(5):363–370.
- Petersen PE, International College of Dentists, WHO. Changing oral health profiles of children in Central and Eastern Europe: challenges for the 21st century. [cited 2020]. Available from: https://www.who.int/oral_health/publications/changing-profiles-children-central-eastern-europe/en/
- Leroy R, Bogaerts K, Martens L, et al. Risk factors for caries incidence in a cohort of Flemish preschool children. Clin Oral Invest. 2012;16(3):805–812.
- de Almeida CM, Petersen PE, Andre SJ, et al. Changing oral health status of 6- and 12-year-old schoolchildren in Portugal. Community Dent Health. 2003;20(4):211–216.
- Vernazza CR, Rolland SL, Chadwick B, et al. Caries experience, the caries burden and associated factors in children in England, Wales and Northern Ireland 2013. Br Dent J. 2016;221(6):315–320.
- Almerich-Silla JM, Montiel-Company JM. Influence of immigration and other factors on caries in 12- and 15-yr-old children. Eur J Oral Sci. 2007;115(5):378–383.
- Du Q, Yu M, Li Y, et al. Permanent caries experience is associated with primary caries experience: a 7-year longitudinal study in China. Community Dent Oral Epidemiol. 2016;45(1):43–48.
- Li Y, Wang W. Predicting caries in permanent teeth from caries in primary teeth: an eight-year cohort study. J Dent Res. 2002;81(8):561–566.
- Hall-Scullin E, Whitehead H, Milsom K, et al. Longitudinal study of caries development from childhood to adolescence. J Dent Res. 2017;96(7):762–767.
- Ekbäck G, Ordell S, Palmetun-Ekbäck M, et al. Reporting dental caries disease in longitudinal studies – a suggestion. Swed Dent J. 2016;40(2):173–179.
- Isaksson H, Alm A, Koch G, et al. Caries prevalence in Swedish 20-year-olds in relation to their previous caries experience. Caries Res. 2013;47(3):234–242.
- Wigen TI, Espelid I, Skaare AB, et al. Family characteristics and caries experience in preschool children. A longitudinal study from pregnancy to 5 years of age. Community Dent Oral Epidemiol. 2011;39(4):311–317.
- Mattila ML, Rautava P, Sillanpaa M, et al. Caries in five-year-old children and associations with family-related factors. J Dent Res. 2000;79(3):875–881.
- Christensen LB, Twetman S, Sundby A. Oral health in children and adolescents with different socio-cultural and socio-economic backgrounds. Acta Odontol Scand. 2010;68(1):34–42.
- Rouxel P, Chandola T. Socioeconomic and ethnic inequalities in oral health among children and adolescents living in England, Wales and Northern Ireland. Community Dent Oral Epidemiol. 2018;46(5):426–434.
- Isaksson H, Koch G, Alm A, et al. Parental factors in early childhood are associated with approximal caries experience in young adults—a longitudinal study. Community Dent Oral Epidemiol. 2019;47(1):49–57.
- Kumar S, Tadakamadla J, Kroon J, et al. Impact of parent-related factors on dental caries in the permanent dentition of 6–12-year-old children: a systematic review. J Dent. 2016;46:1–11.
- Amarante E, Raadal M, Espelid I. Impact of diagnostic criteria on the prevalence of dental caries in Norwegian children aged 5, 12 and 18 years. Commun Dent Oral Epidemiol. 1998;26(2):87–94.
- Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics. 1977;33(1):159–174.
- Batchelor PA, Sheiham A. Grouping of tooth surfaces by susceptibility to caries: a study in 5–16 year-old children. BMC Oral Health. 2004;4(1):2.
- Pitts NB. Are we ready to move from operative to non-operative/preventive treatment of dental caries in clinical practice? Caries Res. 2004;38(3):294–304.
- West P. Health inequalities in the early years: is there equalisation in youth? Soc Sci Med. 1997;44(6):833–858.
- Sjøstrom O, Holst D, Lind SO. Validity of a questionnaire survey: the role of non-response and incorrect answers. Acta Odontol Scand. 1999;57(5):242–246.
- Wigen TI, Baumgartner CS, Wang NJ. Identification of caries risk in 2-year-olds. Community Dent Oral Epidemiol. 2018;46(3):297–302.
- Wigen TI, Wang NJ. Does early establishment of favorable oral health behavior influence caries experience at age 5 years? Acta Odontol Scand. 2015;73(3):182–187.
- The Norwegian Directorate of Health. National guidelines to public health centers and school health services. [cited 2020]. Available from: https://www.helsedirektoratet.no/retningslinjer/helsestasjons-og-skolehelsetjenesten
- The Norwegian Directorate of Health. National guidelines to dental health services for children and adolescents 0-20 years. [cited 2020]. Available from: https://www.helsedirektoratet.no/retningslinjer/tannhelsetjenester-til-barn-og-unge-020-ar