
Abstract
Conclusions: The present study revealed that various etiologies are involved in single-sided deafness (SSD), and that the cause of SSD and asymmetrical hearing loss (AHL) differed greatly between congenital/early-onset cases and adult cases. Clarification of the etiology is the first step toward providing appropriate intervention.
Objectives: The study aimed to clarify the etiology of SSD and AHL patients.
Methods: The etiology of a total of 527 SSD or AHL patients who visited Shinshu University Hospital between 2006 and 2016 were analyzed by imaging as well as serological tests for mumps virus, and CMV DNA testing.
Results: In our cohort of congenital/early-onset SSD (n = 210), the most prevalent cause in children was cochlear nerve deficiency (43.7%; 87 of 199 patients undergoing CT and/or MRI), followed by CMV infection, mumps infection, anomalies of the inner ear, ANSD, and other rare etiologies. In contrast, half of the adult SSD patients presented with idiopathic sensorineural hearing loss, followed by various types of otitis media, cerebellopontine angle tumor and other rare etiologies.
Chinese abstract
结论: 本研究显示, 有各种病因可涉及单侧聋 (SSD) , SSD和不对称听力损失 (AHL) 的原因在先天性/早发性病例和成人病例之间有很大差异。澄清病因是提供适当干预的第一步。
目的: 本研究旨在澄清SSD和AHL患者的病因。
方法: 采用腮腺炎病毒的成像和血清学检测以及CMV DNA检测对在2006年至2016年期间赴Shinshu大学附属医院看病的527例SSD或AHL患者进行了病因学分析。
结果: 在先天性/早发性SSD (n = 210) 病例中, 对于儿童来说, 最常见的原因是耳蜗神经缺乏 (43.7%; 199例中的87例接受了CT和/或MRI) , 其次是CMV感染、内耳异常、ANSD和其它罕见病因。相比之下, 半数成年SSD患者呈现特发性感觉神经性听力损失, 其次是各种类型的中耳炎、小脑蝶碱角瘤和其它罕见的病因。
Introduction
Unilateral hearing loss has been estimated to affect ∼7.9–13.3% of the general population [Citation1,Citation2]. Single-sided deafness (SSD) is the most severe from of unilateral hearing loss, and may lead to social difficulties among patients. For example, SSD had been reported to affect school activities in children, and the emotional or social well-being of adults [Citation3].
Appropriate intervention is, therefore, of great importance, and it is necessary to identify the etiology in order to provide such intervention.
The causes of SSD and asymmetrical hearing loss (AHL) are various, including idiopathic sudden sensorineural hearing loss (SSNHL), acoustic neuroma, anomalies of the inner ear, cochlear nerve deficiency (CND), mumps, congenital cytomegalovirus (CMV) infection, meningitis and auditory neuropathy spectrum disorder (ANSD) [Citation4]. Some cases of SSD and AHL with particular etiologies are progressive in nature. Meanwhile, recent advances in hearing implant technology now enable such patients to enjoy a higher quality of life [Citation5,Citation6, for review]. Thus, appropriate intervention according to etiology is needed. For example, if the etiology is restricted within the inner ear, a cochlear implant is expected to have a good outcome. In contrast, when the etiology is located in the auditory nerve or central auditory system, the outcome is likely to be limited. Therefore, clarification of the etiology is the first step toward providing an appropriate intervention. However, there has been no comprehensive study concerning etiology using consecutive patients. To investigate the etiology of SSD and AHL, we analyzed the etiologies of SSD and AHL using computed tomography (CT), magnetic resonance imaging (MRI), serological as well as DNA testing for viral infection, and genetic testing.
Subjects and methods
Subjects
The subjects used in this study consisted of consecutive patients who visited the ENT Clinic of Shinshu University Hospital between 2006 and 2016.
Audiological classification criteria for asymmetrical hearing loss and single-sided deafness
The inclusion criteria for SSD and AHL used in this study are defined in .
Table 1. Audiological classification criteria for AHL and SSD.
For SSD, 210 congenital/early-onset cases and 182 adult cases (>15 years) were examined in this study. For AHL, seven congenital/early onset cases and 128 adult cases were analyzed.
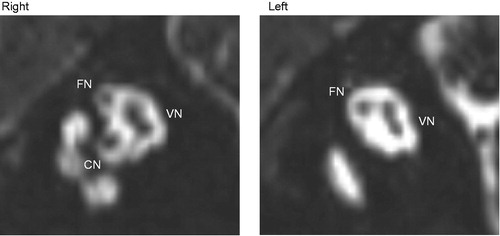
To investigate the etiology, CT and/or MR imaging was performed in 199 out of 217 congenital SSD or AHL cases. Cochlear nerve hypoplasia/deficiency (CND) was diagnosed by MRI or CT, with CND defined as a cochlear nerve canal (CNC) narrower than 1.5 mm () [Citation7]. Parasagittal reconstructions from MR images were used to identify the cochlear nerve () and CND was defined as a cochlear nerve smaller than the facial nerve.
Figure 1. Measurement of the CNC on CT images. The width at the inner margin of its bony walls at the base of the modiolus was measured. The CNC is indicated on the images by arrows.
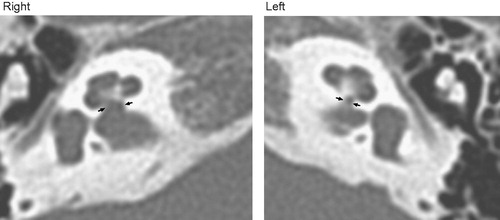
Figure 2. Parasagittal reconstructions from MR images. (Right) Normal, cochlear nerve (CN), facial nerve (FN), superior and inferior vestibular nerve (VN) and (Left) CND.
Presence of an inner ear anomaly was defined according to Sennaroglu’s classification [Citation8].
For diagnosis of congenital CMV infection, real-time polymerase chain reaction (PCR)-based CMV DNA testing using preserved dried umbilical cord specimens was performed. In brief, DNA was extracted from the dried umbilical cord specimens and CMV DNA was amplified and detected by quantitative PCR [Citation9].
For pediatric cases suspected of mumps infection, serological tests for mumps virus were performed. Diagnostic criteria for mumps are shown in .
Table 2. The diagnostic criteria for mumps deafness proposed by the Acute Severe Hearing Loss Study Group, the Ministry of Health, Labor and Welfare of Japan in 1987, and revised in 2013.
For adult SSD/AHL, idiopathic SSNHL was defined as shown in .
Table 3. The diagnostic criteria for idiopathic SSNHL established by the Research Committee of the Ministry of Health, Labour and Welfare of Japan in 2012.
Results
The present results revealed that the causes of SSD differed greatly between congenital/early-onset cases and adult cases ().
Figure 3. (A) The causes of SSD in congenital/early-onset cases. (B) The causes of AHL in congenital/early-onset cases.
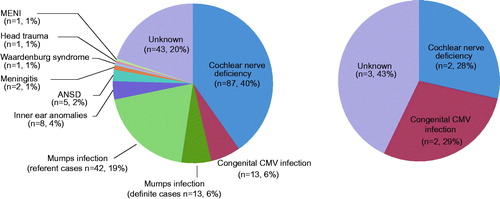
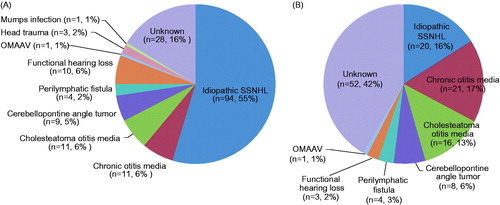
Figure 4. (A) The causes of post-lingual SSD. (B) The causes of post-lingual AHL.
Etiology of the congenital/early onset single-sided deafness and asymmetrical hearing loss cases
In our cohort of congenital/early-onset SSD (n = 216) (), the most prevalent cause in children was CND, with a total frequency of 40% overall; 87/210 (43.7%, 87/199 patients undergoing CT and/or MRI). Among these patients, CND was detected by MRI in 45.9% (51/111) and by CT in 47.6% (81/170) of cases. Five additional cases had associated inner ear anomalies (n = 2) or ANSD (n = 3). The equal second most common causes were CMV infection (6.2% overall; 13/210, 11.5%; 13/113 patients undergoing CMV DNA testing) and mumps infection (6.2%; 13/210 for definite cases, 26.2%; 55/210 including 42 referent cases). Anomalies of the inner ear were found in 3.8% (8/210) of the patients. The most common inner ear anomaly was IP-1 (n = 5), followed by common cavity (n = 3). ANSD was found in 2.4% (5/210) of patients and three additional cases showed accompanying CND. The following causes were also identified: meningitis (1.0%; 2/210), Waardenburg syndrome (0.5%; 1/210), head trauma (0.5%; 1/210) and MENI (0.5%; 1/210). For the rest of the cases (20.5%; 43/210), the cause was unknown.
In the present cohort, the number of patients with congenital/early-onset AHL was limited (n = 7), with CND (n = 2) and CMV (n = 2) identified as the etiology ().
Etiology of the post-lingual single-sided deafness and asymmetrical hearing loss cases
For cases of post-lingual SSD (n = 172) (), idiopathic SSNHL (54.6%; 94/172) was the most common etiology, followed by chronic otitis media (6.4%; 11/172), cholesteatoma otitis media (6.4%; 11/172), functional hearing loss (5.8%; 10/172), cerebellopontine angle tumor (5.2%; 9/172, including six cases of acoustic neuroma), perilymphatic fistula (2.3%; 4/172) and head trauma (1.7%; 3/182). The following etiologies were identified in one case each: mumps, and otitis media with ANCA-associated vasculitis (OMAAV).
For cases of post-lingual AHL (n = 125) (), etiologies similar to SSD were involved: idiopathic SSNHL (16.0%; 20/125), chronic otitis media (16.8%; 21/125), cholesteatoma otitis media (12.8%; 16/125), functional hearing loss (2.4%; 3/125), cerebellopontine angle tumor (6.4%; 8/125, including seven cases of acoustic neuroma), perilymphatic fistula (3.2%; 4/125) and OMAAV (0.8%; 1/125).
Discussion
There have been no comprehensive reports describing the etiology of either pediatric or adult SSD/AHL from various points of view using a large cohort of consecutive cases. The present study clearly indicated that the causes of SSD differ greatly between congenital/early-onset cases and adult cases ( and ).
For congenital/early-onset SSD, it is noteworthy that, if an appropriate set of examinations were carried out, the etiology could be identified or speculated in 80% of cases. CND was the most frequent cause in congenital/early-onset cases in the present cohort. CND may have been underestimated as an etiology for a long time previously, but it has recently been increasingly diagnosed in association with high-resolution MRI. It was recently reported in 55% (6/11) to 26% (33/128) of children with unilateral sensorineural hearing loss (SNHL) [Citation7,Citation10]. The prevalence of CND was much higher (48%) in the subgroup of 50 children with severe or profound hearing loss at diagnosis [Citation10]. The frequency in this study (40% overall, 43.7%; 87/199 in patients undergoing CT and/or MRI) among severe to profound unilateral hearing loss patients was compatible with those reported in the previous studies. In cases with a retro-cochlear pathology, due caution should be exercised when considering cochlear implantation as while it is not a contra-indication, it may limit the outcome [Citation11]. In this study, CND was detected by MRI (45.9%; 51/111) and by CT (47.6%; 81/170). The size of the CNC is somewhat correlated with the presence/absence of the cochlear nerve [Citation7]. CT is beneficial for the diagnosis of middle and inner ear anomalies, whereas MRI is a standard diagnostic tool for identifying the CND.
The equal second most common causes were CMV infection and mumps infection (). CMV infection was found in 6.2% (13/210) of the patients. However, the frequency increased to 11.5% (13/113) when limited to patients for whom CMV DNA testing was performed. Approximately 10% of pediatric cases of SNHL (either bilateral or unilateral) are caused by congenital CMV infection in Japan [Citation9]. According to Furutate et al. (2011) [Citation9], the frequency of congenital CMV infection in children with unilateral SNHL was reported range from 9.1 to 25%. Therefore, the present frequency (11.5%) appears to be compatible with the figures provided in previous reports. Early diagnosis is recommended as the characteristic hearing features have been reported to be progressive [Citation9,Citation12]; therefore, careful follow-up as well as appropriate intervention is needed. Also, as neuro-developmental delay is often associated with hearing impairment, it is recommended that these patients be treated in collaboration with pediatric neurologists [Citation9,Citation12,Citation13].
Mumps infection was also a frequent cause for congenital/early-onset SSD cases in this study (definite cases 6.2%; 13/210). If referent cases (n = 42) are included, the frequency increases to 26.2%. The present study clearly indicated that a significant number of patients in Japan had unilateral hearing loss due to mumps infection (). A national survey has indicated that a significant number of patients still suffer from mumps [Citation14, also Morita et al.]. Mumps vaccination is routinely performed as part of a national immunization program in many countries. These countries have shown a rapid decline in mumps morbidity, and mumps-associated encephalitis and deafness have nearly vanished [Citation15]. Despite these facts, the use of measles–mumps–rubella (MMR) vaccine remains optional in Japan [Citation14], posing an urgent problem that needs to be resolved.
Inner ear anomalies were found in 3.8% (8/210) of congenital/early-onset SSD cases and 4.0% (8/199) of the patients for whom imaging evaluation was performed. Incomplete partition type-I (IP-I) (5/8) was the most frequent inner ear malformation, followed by common cavity (3/8). Previous studies have demonstrated that inner ear malformations in SSD children are found in ∼25–35% of cases by CT or MRI [Citation16,Citation17]. The algorithm for the detection of inner ear malformations in SSD children remains controversial [Citation16]. In this cohort, there was no uniform algorithm applied; therefore, future prospective studies will be needed. Nevertheless, it is generally accepted that CT is more suited to the identification of inner and middle ear anomalies, whereas MRI is more beneficial in the detection of CND [Citation7,Citation8,Citation16,Citation17].
ANSD was found in 2.4% (5/210) of congenital/early-onset SSD cases. Three cases were associated with CND. Previous studies pointed out that CND is one of the etiologies of auditory neuropathy [Citation18].
As expected, we identified very few cases with hearing loss due to genetic causes. It is well-known that ∼60% of cases of congenital or early-onset bilateral hearing loss are attributable to genetic causes [Citation19]. On the other hand, most cases of unilateral hearing loss are not attributable to genetic causes. Waardenburg syndrome, however, is an exception as this syndrome may show either bilateral or unilateral sensorineural hearing loss [Citation20]. In fact, one patient with Waardenburg syndrome presented with SSD in our cohort.
For post-lingual SSD, the present results indicated that idiopathic SSNHL (54.6%) was the most common etiology, followed by various forms of otitis media including chronic otitis media, cholesteatoma otitis media and OMAAV. Functional hearing loss and cerebellopontine angle tumor, which should be included as a different diagnosis, were also important causes of SSD among adult patients.
For cases of post-lingual AHL, there were fewer cases of idiopathic SSNHL (16.0%) in comparison with the SSD group, while other acquired etiologies, such as various types of otitis media, functional hearing loss, cerebellopontine angle tumor and perilymphatic fistula, were identified at similar rates to those in the SSD group.
With regard to intervention, it should be noted that hearing implant technology has been progressing rapidly, with post-lingual idiopathic SSNHL, in particular, being one of etiologies most likely to benefit from cochlear implantation. On the basis of speech recognition testing, sound localization testing and tinnitus handicap questionnaire, a series of studies regarding CI outcomes in cases of SSD caused by idiopathic SSNHL have indicated that CI is beneficial for these patients [Citation5,6, for review].
In contrast, for congenital/early-onset SSD, due caution is required in that the most prevalent etiology, based on radiological evaluation, appears to be CND or hypoplasia. Naturally, cochlear nerve function is a key prognostic factor for a good outcome after CI. Therefore, the etiology should be considered when deciding whether CI would applicable for SSD and AHL patients. Although further evaluation using a large number of the patients is needed, recent case series have suggested that improvement in speech perception in noise and sound localization ability is possible, although the results varied from patient to patient [Citation11]. Bone conduction devices and contralateral routing of sound systems are also worthy of consideration for SSD patients [Citation6].
In conclusion, the present study revealed that various etiologies are involved in SSD and AHL. Further, the etiology differed greatly between congenital/early-onset cases and adult cases, and clarification of the etiology is becoming more and more crucial to the provision of appropriate intervention.
Acknowledgements
This study was supported by a Health and Labour Sciences Research Grant for Comprehensive Research on Disability Health and Welfare from the Ministry of Health, Labour and Welfare, Japan (http://www.mhlw.go.jp/english/) (S.U.).
Disclosure statement
The authors report no conflicts of interest. The authors alone are responsible for the content and writing of this article. The Shinshu University Conflict of Interest Committee also approved the study.
Additional information
Funding
References
- Chia EM, Wang JJ, Rochtchina E, Cumming RR, Newall P, Mitchell P. Hearing impairment and health-related quality of life: the Blue Mountains Hearing Study. Ear Hear 2007;28:187–95.
- Agrawal Y, Platz EA, Niparko JK. Prevalence of hearing loss and differences by demographic characteristics among US adults: data from the National Health and Nutrition Examination Survey, 1999-2004. Arch Intern Med 2008;168:1522–30.
- Iwasaki S, Sano H, Nishio S, Takumi Y, Okamoto M, Usami S, et al. Hearing handicap in adults with unilateral deafness and bilateral hearing loss. Otol Neurotol 2013;34:644–9.
- Vila P, Judith E, Lieu C. Asymmetric and unilateral hearing loss in children. Cell Tissue Res 2015;361:271–8.
- Cabral Junior F, Pinna MH, Alves RD, Malerbi AFS, Bento RF, et al. Cochlear implantation and single-sided deafness: a systematic review of the literature. Int Arch Otorhinolaryngol 2016;20:69–75.
- Kitterick PT, Smith SN, Lucas L. Hearing instruments for unilateral severe-to-profound sensorineural hearing loss in adults: a systematic review and meta-analysis. Ear Hear 2016;37:495–507.
- Miyasaka M, Nosaka S, Morimoto N, Taiji H, Masaki H. CT and MR imaging for pediatric cochlear implantation: emphasis on the relationship between the cochlear nerve canal and the cochlear nerve. Pediatr Radiol 2010;40:1509–16.
- Sennaroglu L, Saatci I. A new classification for cochleovestibular malformations. Laryngoscope 2002;112:2230–41.
- Furutate S, Iwasaki S, Nishio SY, Moteki H, Usami S. Clinical profile of hearing loss in children with congenital cytomegalovirus (CMV) infection: CMV DNA diagnosis using preserved umbilical cord. Acta Otolaryngol 2011;131:976–82.
- Clemmens CS, Guidi J, Caroff A, Cohn SJ, Brant JA, Laury AM, et al. Unilateral cochlear nerve deficiency in children. Otolaryngol Head Neck Surg 2013;149:318–25.
- Arndt S, Prosse S, Laszig R, Wesarg T, Aschendorff A, Hassepass F. Cochlear implantation in children with single-sided deafness: does aetiology and duration of deafness matter? Audiol Neurootol 2015;20(Suppl. 1):21–30.
- Rosenthal LS, Fowler KB, Boppana SB, Britt WJ, Pass RF, Schmid DS, et al. Cytomegalovirus shedding and delayed sensorineural hearing loss: results from longitudinal follow-up of children with congenital infection. Pediatr Infect Dis J 2009;28:515–20.
- Inaba Y, Motobayashi M, Nishioka M, Kaneko T, Yamauchi S, Kawasaki Y, et al. Correlation between white matter lesions and intelligence quotient in patients with congenital cytomegalovirus infection. Pediatr Neurol 2016;55:52–7.
- Kawashima Y, Ihara K, Nakamura M, Nakashima T, Fukuda S, Kitamura K. Epidemiological study of mumps deafness in Japan. Auris Nasus Larynx 2005;32:125–8.
- Galazka AM, Robertson SE, Kraighter A. Mumps and mumps vaccine: a global review. Bull World Health Organ 1999;77:3–14.
- Simons JP, Mandell DL, Arjmand EM. Computed tomography and magnetic resonance imaging in pediatric unilateral and asymmetric sensorineural hearing loss. Arch Otolaryngol Head Neck Surg 2006;132:186–92.
- Song JJ, Choi HG, Oh SH, Chang SO, Kim CS, Lee JH. Unilateral sensorineural hearing loss in children: the importance of temporal bone computed tomography and audiometric follow-up. Otol Neurotol 2009;30:604–8.
- Kim SH, Choi HS, Han YE, Choi BY. Diverse etiologies manifesting auditory neuropathy characteristics from infants with profound hearing loss and clinical implications. Int J Pediatr Otorhinolaryngol 2016;86:63–7.
- Morton CC, Nance WE. Newborn hearing screening-a silent revolution. N Engl J Med 2006;354:2151–64.
- Kim SH, Kim AR, Choi HS, Kim MY, Chun EH, Oh SH, et al. Molecular etiology of hereditary single-side deafness: its association with pigmentary disorders and Waardenburg syndrome. Medicine (Baltimore) 2015;94:e1817.