
Abstract
Background: β-adrenergic signaling has been implicated in the pathology of hepatocellular carcinoma (HCC), but the evidence from clinical studies is limited. In this national population-based cohort study, we investigated the possible association of β-adrenergic receptor blockers and cancer-specific mortality among patients with primary HCC diagnosed in Sweden between 2006 and 2014.
Methods: Patients were identified from the Swedish Cancer Register (n = 2104) and followed until 31 December 2015. We used Cox regression to evaluate the association of β-blockers dispensed within 90 days prior to cancer diagnosis, ascertained from the national Prescribed Drug Register, with liver cancer mortality identified from the Cause of Death Register, while controlling for socio-demographic factors, tumor characteristics, comorbidity, other medications and treatment procedures.
Results: Over a median follow-up of 9.9 months, 1601 patients died (of whom 1309 from liver cancer). Compared with non-use, β-blocker use at cancer diagnosis [n = 714 (predominantly prevalent use, 93%)] was associated with lower liver cancer mortality [0.82 (0.72–0.94); p = .005]. Statistically significant associations were observed for non-selective [0.71 (0.55–0.91); p = .006], β1-receptor selective [0.86 [0.75–1.00); p = .049] and lipophilic [0.78 (0.67–0.90); p = .001] β-blockers. No association was observed for hydrophilic β-blockers [1.01 (0.80–1.28); p = .906] or other antihypertensive medications. Further analysis suggested that the observed lower liver cancer mortality rate was limited to patients with localized disease at diagnosis [0.82 (0.67–1.01); p = .062].
Conclusion: β-blocker use was associated with lower liver cancer mortality rate in this national cohort of patients with HCC. A higher-magnitude inverse association was observed in relation to non-selective β-blocker use.
Introduction
Liver cancer is one of the leading causes of cancer-related mortality worldwide [Citation1]. Despite improving survival trends [Citation2], the prognosis of liver cancer is poor with worldwide 5-year net survival estimates ranging from 5 to 30% [Citation2].
A growing body of evidence suggests a role of β-adrenergic signaling in tumor biology, and links β-adrenergic-receptor blockers with reduced cancer progression, especially in early-stage disease [Citation3], via inhibition of various cancer-related cellular and molecular processes involved in sympathetic nervous system (SNS) activation [Citation4]. However, associations with mortality vary by tumor site [Citation5,Citation6] and subtype [Citation7,Citation8].
The predominant adrenoreceptors expressed in the human liver are of the α1- and β2-subtypes [Citation9,Citation10]. β2-adrenoreceptors have been shown to mediate noradrenaline/adrenaline-induced cell invasion and anoikis inhibition in hepatocellular carcinoma (HCC) [Citation11], the most common type of primary liver cancer, and β2-adrenergic receptor signaling has been linked to sustained HCC cell proliferation and survival [Citation12]. A higher density of β2-adrenoreceptors has further been detected in HCC tissue than in the nonadjacent non-tumor liver tissue [Citation13,Citation14]. The β2-adrenoreceptor upregulation has in turn been associated with clinico-pathological factors including large tumor size, vascular invasion, poor differentiation, and poor prognosis [Citation15]. Further, the most frequently investigated β-blocker, propranolol, has been shown to inhibit proliferation, promote apoptosis, induce S-phase arrest [Citation16], and reduce invasion and migration [Citation17] in liver cancer cells. A meta-analysis of randomized trials on non-selective β-blockers for prevention of variceal bleeding in patients with liver cirrhosis has linked non-selective β-blockers with reduced risk of HCC but not HCC mortality [Citation18]. However, the meta-analysis was limited by a small number of patients and events, mainly because the majority of eligible trials did not register HCC incidence or HCC mortality [Citation18]. The evidence from studies designed to study the association of β-blocker use with liver cancer survival is still scarce. In a small (n = 36) retrospective study of adults with non-metastatic HCC, β-blocker use has been associated with improved overall survival [Citation19]. In a population-based study using the National Health Insurance Research Database of Taiwan, propranolol was associated with improved overall survival in unresectable/metastatic HCC [Citation20].
In this large population-based cohort of patients with primary HCC, we therefore tested the hypothesis that β-blocker use at cancer diagnosis may reduce liver cancer mortality rate.
Patients and methods
Study population and data sources
We used prospectively collected data available through national Swedish registers to conduct this retrospective cohort study. The unique personal identification number assigned to all Swedish residents was used to perform individual record linkage.
From the Swedish Cancer Register [Citation21], we identified patients (aged 18 years or older) diagnosed with first primary liver cancer between 1 January 2006, and 31 December 2014, using the International Classification of Diseases (ICD) 7th revision code 155.0, and obtained information on tumor stage and histology, year of diagnosis, and age at diagnosis.
Prescriptions of β-blockers, as well as other relevant medications dispensed during the 90-day period before liver cancer diagnosis were identified from the Prescribed Drug Register [Citation22] using the Anatomic Therapeutic Chemical (ATC) classification system. The number of distinct medication classes (medications with the same initial five characters of the ATC classification) was used to derive a medication-based comorbidity score to account for overall disease burden [Citation23,Citation24]. Post-diagnostic collection of a prescription for sorafenib, a kinase inhibitor used in advanced-stage liver cancer, was also identified.
The Patient Register [Citation25] provided data on specific comorbidity, liver resection, liver transplantation and loco-regional therapies such as ablation and transarterial chemoembolization (TACE) (Supplementary Table S1). The Total Population Register provided migration data, while the LISA (Swedish acronym for Longitudinal Database of Education, Income and Occupation) [Citation26] was used to ascertain the level of attained education, marital status and region of residence. The Cause of Death Register [Citation27] provided information on the underlying cause of death.
We excluded patients with liver cancer other than HCC identified through the ICD-O-3 morphological code 81703 (Supplementary Figure S1).
β-Blocker exposure assessment
Patients were classified as exposed at the time of cancer diagnosis if they had collected β-blockers from the pharmacy any time during the 90 days preceding their cancer diagnosis, as prescriptions normally cover a period of 30 to 90 days (maximum 1 year) in Sweden. β-blocker exposure was further defined by receptor selectivity [nonselective (ATC codes: C07AA and C07AG), selective (C07AB and C07FB02)], and solubility (lipophilic, hydrophilic). Patients using both selective and non-selective β-blockers were placed in the non-selective subgroup, while users of both lipophilic and hydrophilic types were included in the lipophilic subgroup. Where possible, associations with individual β-blockers were investigated.
β-blocker use was also classified as incident or prevalent in a sensitivity analysis performed in 1965 patients diagnosed on or after 1 October 2006, where use was defined as incident if patients collected their β-blockers from the pharmacy within 90 days before cancer diagnosis date, but had no recorded collection in the previous year.
Outcome assessment
Cancer-specific mortality (CSM) was identified from the Causes of Death Register using ICD-10 code C22 capturing cancer of the liver including intrahepatic cholangiocarcinoma. Patients were followed from the date of cancer diagnosis until date of emigration, death, or 31 December 2015, whichever came first.
Statistical analysis
Patient characteristics were tabulated by β-blocker use and compared using the χ², ANOVA or median tests as appropriate. The observed 6-month, 1-year, and 5-year overall survival proportions were estimated using the actuarial method. Flexible parametric survival analysis (baseline hazards were modeled using splines with five degrees of freedom) [Citation28] was applied to estimate age-adjusted median survival and liver cancer survival curves by β-blocker use. The multivariable fractional polynomials method [Citation29] assessed the functional form of continuous variables in the log-hazard function. Cox regression models with time since diagnosis in months as the underlying time scale were fitted to estimate hazard ratios (HR) and 95% confidence intervals (CI) for the β-blocker-CSM association. Test and plots of Schoenfeld residuals evaluated the proportional hazards assumption, which was satisfied for β-blockers.
Multivariable Cox regression models included age at cancer diagnosis, the medication-based comorbidity score, and year of diagnosis modeled as linear measures; sex; attained education [categories by duration: compulsory (up to 9 years), secondary (10–12 years), and postsecondary (more than 12 years); marital status [categories: unmarried, married/cohabiting, divorced/separated, or widowed]; region of residence; tumor–node–metastasis (TNM) stage [classified into stages 1–4B (Supplementary Table S2)]; specific comorbid diseases at liver cancer diagnosis [portal vein thrombosis, diabetes, gastro-esophageal varices with and without bleeding, viral hepatitis C and other types, diseases of liver under ICD-10: K70-K77 capturing fibrosis/cirrhosis of the liver and other conditions] and specific medications [loop diuretics, other antihypertensive medications, NSAIDs, aspirin and statins]. To identify presence of liver decompensation not identifiable through ICD codes in the data, we included use of spironolactone and lactulose as indicators of cirrhotic ascites and hepatic encephalopathy, respectively. A further adjusted model (referred to as fully adjusted) included some other indicators of liver function such as alcohol abuse-related morbidity at diagnosis (more relevant in the Nordic countries [Citation30], as well as ablation, TACE, liver resection, liver transplantation and sorafenib use. Ablation, TACE, liver resection, liver transplantation, sorafenib use as well as portal vein thrombosis were modeled as time-varying covariates in the fully adjusted model using time dependent Cox regression. Multiplicative interaction terms were added to the fully adjusted model to test whether associations differ by sex. In a sensitivity analysis, we further adjusted for cardiovascular diseases. Besides analyses in all HCC patients, analyses stratified by known distant metastases at diagnosis (M stage at diagnosis recorded as M0 or M1) were conducted.
Since patients with cirrhosis who have developed hepatorenal syndrome have been recommended to discontinue or avoid β-blocker use [Citation31], we performed a sensitivity analysis where patients with likely hepatorenal morbidity [identified through ICD codes for moderate-to-severe renal disease and diseases under ICD-10 K76 code, which captures hepatorenal syndrome (K76.7)] were excluded. As it has been suggested that non-selective β-blockers may be associated with reduced survival in patients with hepatic decompensation/refractory ascites [Citation31], we performed an exploratory analysis among patients likely to have decompensated liver disease. This subgroup of patients was identified based on diagnoses of hepatic failure (ICD-10: K72) or bleeding varices, or dispensed prescriptions of lactulose or spironolactone. In another sensitivity analysis among 1479 patients diagnosed on or after 1 July 2006, we compared with non-use the use of selective β-blockers and other antihypertensive medications dispensed for no other indication but hypertension (as specified in the Prescribed Drug Register). Prior prescriptions dispensed during 1 year before cancer diagnosis also had to be for no other indication but hypertension.
All analyses were performed using Stata version 14/SE for Windows (StataCorp) software. The study was approved by an ethical review board in Uppsala (DNR: 2012-361).
Results
Study population and overall survival estimates
The analytic cohort included 2104 patients with primary HCC. The median age at diagnosis was 68 years (range: 30–94 years). The cancer diagnosis was based on histopathology (73.4%); X-ray, scintigraphy, ultrasound, magnetic resonance imaging, computed tomography, or equivalent (3.0%); cytology (6.3%); or other laboratory tests (17.2%). About half (51.4%) of the patients had no known distant metastases at diagnosis. Patients with pre-existing liver morbidity (n = 984) were more likely to be diagnosed at early stages.
Over a total observation period of about 3316 person-years, 1601 (76.1%) patients died, another 7 (0.3%) emigrated, and 496 (23.6%) were followed to the end of the study. The causes of death were liver cancer (n = 1309), other tumors (n = 84), cardiovascular disease (n = 55), or other causes (n = 153) including chronic viral hepatitis (n = 38) and diseases of liver (n = 46)]. The median survival was 9.9 months.
The estimated 6-month, 1-year, and 5-year overall survival proportions were 59, 46, and 19%, respectively. The corresponding estimates were 59, 45, 19% for non-users; 55, 42, 13% for selective β-blocker users and 74, 62, 35% for non-selective β-blocker users.
β-Blocker use
Overall, 714 (34%) patients used β-blockers at the time of liver cancer diagnosis. Most commonly prescribed β-blockers belonged to the β1-cardio-selective type (68.1%), consisting predominantly of lipophilic metoprolol, while non-selective β-blockers comprised 33.9% and consisted mainly of lipophilic propranolol (Supplementary Table S3). Only 15 (2.1%) users received agents belonging to different β-blocker classes (for example, both selective and non-selective). β-Blockers with partial agonist activity were very rare.
The majority (about 93% of users) had received β-blockers also before the 90-day exposure window used by the study. Only a few (38 users of non-selective and 24 users of selective types) met the incident user definition for a sensitivity analysis performed in patients diagnosed on or after 1 October 2006.
In general, β-blocker users were more likely to be married/cohabiting and had a higher comorbidity score. Compared with users of selective β-blockers or non-users, users of non-selective types tended to be younger and more likely to be diagnosed with portal vein thrombosis, gastroesophageal varices, viral hepatitis, and various liver diseases [particularly, alcoholic liver disease (ICD-10: K70), hepatic failure (K72), fibrosis/cirrhosis of liver (K74), and other diseases of liver (K76)] as well as to be diagnosed at early stages of cancer (). Medications associated with cirrhotic ascites and hepatic encephalopathy were also more common among non-selective β-blocker users. Users of selective β-blockers had fewer years of education and were more likely to be diagnosed with diabetes, moderate-to-severe renal disease and cardiovascular diseases other than varices and portal vein thrombosis (for example, coronary artery disease, chronic heart failure and cerebrovascular disease). Other antihypertensive medications were also more common among users of selective β-blockers.
Table 1. Baseline characteristics of patients diagnosed with primary hepatocellular carcinoma in Sweden in 2006 to 2014 by β-blocker use at cancer diagnosis.
β-Blocker use and liver cancer specific mortality
The CSM rates (per 100 person-months) were lower among β-blocker users than non-users [2.85 (2.59–3.14) and 3.54 (3.32–3.78), respectively] with a corresponding statistically significant HR of 0.85 (0.76–0.96; p = .007). Further analysis suggested that the lower CSM rates among users were driven by rates among users of non-selective [1.51 (1.25–1.83)] rather than selective [4.09 (3.66–4.57)] β-blockers.
In age-adjusted analyses, any β-blocker use was associated with a 19% lower CSM (, ). The estimates remained largely unchanged and statistically significant after further multivariable adjustments (). Additional adjustment for cardiovascular diseases (main indications for β-blocker use, particularly selective types) did not affect the results.
Figure 1. Age-adjusted liver cancer survival curves by β-blocker use among patients with primary hepatocellular carcinoma diagnosed in 2006 to 2014 in Sweden. Survival curves were estimated using flexible parametric survival analysis. The adjusted curves show the survival we would expect to see in exposure groups if each had the age distribution of the study population as a whole (to compare like with like). Values on the plot are age-adjusted median survival estimates by β-blocker use.
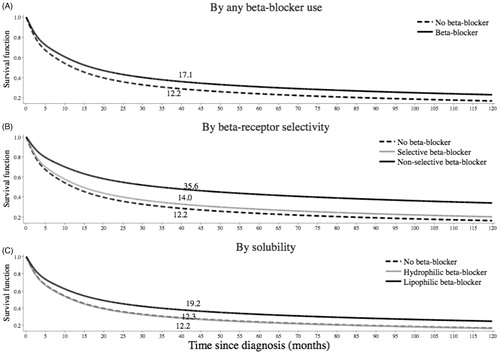
Table 2. Cox proportional hazards regression analyses for the association between β-blocker use and liver cancer mortality in patients diagnosed with primary hepatocellular carcinoma (N = 2104) in Sweden in 2006–2014.
Analyses differentiating β-blockers by receptor selectivity suggested higher-magnitude associations for non-selective β-blockers, although the difference between the estimates was not statistically significant (p = .143) (). The hazard ratio for the association between non-selective β-blocker use and CSM was not significantly altered after adjustment for diagnosis of gastroesophageal varices, the most common indication for non-selective β-blocker treatment, although some attenuation of the inverse association was observed.
Analyses by solubility further indicated lower CSM for lipophilic but not hydrophilic β-blocker use (difference between the estimates: p = .036) (). There were no notable differences between men and women.
Results for selected individual β-blockers were consistent with results for β-blocker types evaluated in aggregate (). Non-selective and highly lipophilic propranolol was associated with a statistically significant 28% lower mortality rate, and commonly prescribed β1-selective and highly lipophilic metoprolol was associated with a 19% lower mortality rate. A higher magnitude association (48% lower mortality rate) was observed for the less often prescribed carvedilol, a moderately lipophilic and non-selective β-blocker with anti-α1 adrenergic activity. Use of moderately lipophilic bisoprolol or hydrophilic atenolol, both with higher (compared with metoprolol) β1-selectivity, did not show associations with CSM.
Table 3. Cox proportional hazards regression analyses for the association between selected β-blockers and liver cancer mortality in patients diagnosed with primary hepatocellular carcinoma (N = 2104) in Sweden in 2006–2014.
In our sensitivity analysis we observed similar magnitude associations for incident and prevalent use of non-selective β-blockers [0.71 (0.44–1.14) vs. 0.70 (0.53–0.93)] as well as for incident and prevalent use of selective β-blockers [0.87 (0.52–1.46) vs. 0.83 (0.71–0.97)].
Stratified analyses suggested a lower CSM among patients without known distant metastases at diagnosis [0.82 (0.67–1.01), p = .062], whereas the magnitude of association was close to null in patients with distant metastases [0.98 (0.71–1.36), p = .910].
In exploratory analyses among 655 patients with indications of decompensated liver disease, non-selective β-blockers were still associated with lower CSM [0.73 (0.50–1.05), p = 0.089)] although statistical significance was not achieved. Further analysis suggested an inverse association for propranolol [n = 155; HR: 0.67 (0.46, 0.98)] but not for the rarely used carvedilol [n = 5; HR: 1.33 (0.39, 4.55)]. The magnitude of association was close to null for selective β-blockers [0.98 (0.72–1.33)].
Non-selective β-blockers were associated with lower CSM [0.68 (0.51–0.90), p = .007] also in a sensitivity analysis excluding 363 patients with hepatorenal morbidity. A lower magnitude association was observed in relation to selective types [0.85 (0.73–1.00), p = .055].
In a sensitivity analysis excluding patients who used β-blockers and/or other antihypertensive medications dispensed for indications other than hypertension, selective β-blockers were associated with lower CSM, while other antihypertensive medications were not ().
Table 4. Cox proportional hazards regression analyses for the association between antihypertensive medications and liver cancer mortality in patients diagnosed with primary hepatocellular carcinoma in Sweden between 1 July 2006 and 31 December 2014 (N = 1479).
Discussion
In this large population-based cohort of patients with primary HCC, β-blocker use at cancer diagnosis was associated with lower liver cancer specific mortality. The reduced liver cancer mortality rate was limited to patients without known distant metastases at diagnosis. Higher-magnitude inverse associations were suggested for non-selective than selective β-blockers, and the association was apparent for lipophilic but not hydrophilic β-blockers.
HCC typically arises in the background of cirrhosis and only about 20% of HCCs have been reported to develop in non-cirrhotic livers [Citation32]. While tumor recurrence is the major cause of death in non-cirrhotic HCC [Citation32], patients with HCC in cirrhotic liver often die from complications of liver cirrhosis and portal hypertension rather than from clearly tumor-related causes. Non-selective β-blockers are recommended for patients with cirrhosis and esophageal varices to prevent variceal hemorrhage [Citation33,Citation34]; and have been shown to lower the risk of spontaneous bacterial peritonitis in patients with cirrhosis and ascites [Citation35] and risk of developing ascitic decompensation, refractory ascites and hepatorenal syndrome in patients with compensated cirrhosis [Citation36]. Improved survival associated with non-selective β-blockers may thus be partly explained by reduced risk of hepatic decompensation-related mortality. Unlike non-selective β-blockers, selective β-blockers are more likely prescribed to patients with compensated liver who thus have a better liver function related prognosis irrespective of β-blocker use.
Increased surveillance of patients with cirrhosis leading to earlier cancer detection [Citation37] may offer another potential explanation. This is less likely among patients with non-cirrhotic HCC as they are often diagnosed at an advanced stage due to lack of surveillance [Citation32].
A growing body of evidence has suggested a role of β-adrenergic signaling in the pathobiology of various tumor types [Citation4], including liver cancer [Citation11,Citation12,Citation15–17,Citation19,Citation38], and the observed lower CSM rates among β-blocker users could also be related to reduced cancer progression linked to inhibited β-adrenergic signaling. The observed inverse association between CSM and use of selective β-blockers but not other antihypertensive medications dispensed for hypertension may add some additional suggestive evidence for the role of β-adrenergic signaling in HCC pathology.
A lower mortality rate among patients without distant metastases is consistent with the concept of greater influence of biobehavioral factors in early stage cancer when the metastatic capacity is physiologically modifiable [Citation3], although some benefit even for late-stage disease may exist due to treatment-sensitizing effects of β-blockers [Citation39].
It has been suggested that the β2-adrenoreceptor is the adrenoreceptor most involved in cancer related processes [Citation40], including for liver-cancer [Citation11,Citation12,Citation15,Citation38]; and that propranolol, shown to have antiproliferative, antimigratory, and cytotoxic properties [Citation16,Citation17], may be more cytotoxic for liver cancer cells than atenolol [Citation17]. This could potentially partially explain the higher-magnitude associations with non-selective β-blockers (comprised mainly of propranolol in this cohort). However, β1- and β2-receptors are in general very similar, and the majority of β-blockers used in clinical practice (including metoprolol and atenolol) show little selectivity for the β1- over the β2-adrenoreceptor [Citation41]. Our results further suggested an association of lipophilic β-blockers with reduced CSM, while no association was observed for hydrophilic β-blockers. As lipophilic agents have greater penetrance of the blood-brain barrier, this finding may suggest that some of the hypothesized anti-tumor effects of β-blockers may be mediated through central β-adrenergic signaling [Citation4]. Carvedilol, a non-selective β-blocker with anti-α1 adrenergic activity, which demonstrated higher magnitude associations in our study overall, has been studied as a promising β-blocker in liver pathology [Citation31,Citation34], but perhaps not among patients with severe or refractory ascites [Citation31].
Strengths of this study include use of high-quality prospectively collected data from national registers in the setting of a tax-supported universal health care system, minimizing the risk of selection bias, and substantially reducing the likelihood of the findings being confounded by socioeconomic characteristics.
Defining exposure to medications through dispensed prescriptions prevents problems such as recall bias or failure to fill prescribed medication (a key component of non-adherence). However, exposure misclassification is still possible, and a prescription filled does not guarantee that the dispensed medication has been used. Although the information on medication compliance is unavailable, the requirement for patients to pay a component of the dispensed price should increase the probability of actual use. Our definition of exposure does not account for potential changes in use during follow-up, but resembles the intention-to-treat analysis in randomized studies and eliminates the possibility of immortal time bias. Besides studying β-blockers in aggregate, we studied some individual β-blockers with varying β-receptor ligand selectivity and lipophilicity/hydrophilicity. However, these analyses are limited by low prevalence of some β-blockers. For example, the low prevalence of hydrophilic sotalol and lack of lipophilic timolol, both with higher β2-selectivity compared to propranolol [Citation41], limits the possibility to make inferences regarding relative importance of β2-selectivity level and solubility of non-selective types. As the medication data are only available since the start of the register in July 2005, we were unable to evaluate the role of duration of β-blocker use [Citation42], the significance of which is largely unknown [Citation43]. Since comparison of prevalent users with non-users could be subject to selection bias [Citation44], we examined associations for incident and prevalent β-blocker use compared with non-use. This analysis, although limited by a small number of incident users, did not reveal any clear differences between estimates for incident and prevalent use.
Due to the observational nature of the study, the possibility of residual confounding cannot be excluded, and confounding by indication [Citation45] or by liver functional status is possible. Although the national register data allowed us to account for a number of important potential confounding and prognostic factors, the data was limited by the absence of stage information according to Barcelona-Liver Cancer (BCLC) staging system, one of the most widely used classifications for HCC in cirrhotic liver that accounts not only for tumor extent but also for other determinants of prognosis such as liver function and performance status [Citation46]. The nature of the registry data limited our ability to accurately identify all patients with and without underlying cirrhosis and to adjust for severity of cirrhosis through Child-Pugh score or other specific measures of the underlying liver function [Citation46]. Nevertheless, the inability to efficiently adjust for performance status and cirrhosis severity could explain the observed inverse associations if patients with poor performance status and more advanced liver impairment, who tend to have worse prognosis, were less likely to take β-blockers, for example, patients with cirrhosis who have developed hepatorenal syndrome [Citation31,Citation47]. However, excluding patients with hepatorenal morbidity did not affect the results. As β-blocker users tended to be older and with higher disease burden, the observed inverse association with CSM is less likely to be explained by selective avoidance of prescribing β-blockers to frail patients. Furthermore, patients on non-selective β-blockers generally have more advanced portal hypertension with large gastroesophageal varices [Citation47].
In conclusion, β-adrenergic receptor blockers, particularly non-selective types, are associated with lower liver cancer mortality in patients with primary HCC. Various potential mechanisms could explain the observed inverse association, including an influence on hepatic decompensation-related mortality as well as early detection of cancer due to active surveillance (particularly among patients with HCC in cirrhotic liver). Reduced cancer progression due to β-adrenergic signaling inhibition could be another potential explanation. Further clinicopathological investigations are necessary to disentangle potential mechanisms. Thus, the role of β-blockers, particularly propranolol, in HCC progression could be an area for further investigation, but the findings from pre-clinical and observational studies need to be verified by prospective clinical trials.
Ethical approval
Ethical review board in Uppsala (DNR: 2012-361).
Supplemental Material
Download PDF (182.6 KB)Acknowledgement
The funder of the study had no role in the study design, data analyses, interpretation or writing of the manuscript. Ann-Sofi Duberg has given lectures with honoraria and/or been consultant to AbbVie, BMS, Gilead, Janssen, MSD.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–386.
- Allemani C, Matsuda T, Di Carlo V, et al. Global surveillance of trends in cancer survival 2000-14 (CONCORD-3): analysis of individual records for 37 513 025 patients diagnosed with one of 18 cancers from 322 population-based registries in 71 countries. Lancet. 2018;391(10125):1023–1075.
- Costanzo ES, Sood AK, Lutgendorf SK. Biobehavioral influences on cancer progression. Immunol Allergy Clin North Am. 2011;31(1):109–132.
- Cole SW, Sood AK. Molecular pathways: beta-adrenergic signaling in cancer. Clin Cancer Res. 2012;18(5):1201–1206.
- Choi CH, Song T, Kim TH, et al. Meta-analysis of the effects of beta blocker on survival time in cancer patients. J Cancer Res Clin Oncol. 2014;140(7):1179–1188.
- Weberpals J, Jansen L, Carr PR, et al. Beta blockers and cancer prognosis – the role of immortal time bias: a systematic review and meta-analysis. Cancer Treat Rev. 2016;47:1–11.
- Melhem-Bertrandt A, Chavez-Macgregor M, Lei X, et al. Beta-blocker use is associated with improved relapse-free survival in patients with triple-negative breast cancer. JCO. 2011;29(19):2645–2652.
- Botteri E, Munzone E, Rotmensz N, et al. Therapeutic effect of beta-blockers in triple-negative breast cancer postmenopausal women. Breast Cancer Res Treat. 2013;140(3):567–575.
- Kawai Y, Powell A, Arinze IJ. Adrenergic receptors in human liver plasma membranes: predominance of beta 2- and alpha 1-receptor subtypes. J Clin Endocrinol Metab. 1986;62(5):827–832.
- Kassahun WT, Gunl B, Tannapfel A, et al. Alpha1-and beta2-adrenoceptors in the human liver with mass-forming intrahepatic cholangiocarcinoma: density and coupling to adenylate cyclase and phospholipase C. Naunyn Schmied Arch Pharmacol. 2005;372(3):171–181.
- Li J, Yang XM, Wang YH, et al. Monoamine oxidase A suppresses hepatocellular carcinoma metastasis by inhibiting the adrenergic system and its transactivation of EGFR signaling. J Hepatol. 2014;60(6):1225–1234.
- Wu FQ, Fang T, Yu LX, et al. ADRB2 signaling promotes HCC progression and sorafenib resistance by inhibiting autophagic degradation of HIF1alpha. J Hepatol. 2016;65(2):314–324.
- Bevilacqua M, Norbiato G, Chebat E, et al. Changes in alpha-1 and beta-2 adrenoceptor density in human hepatocellular carcinoma. Cancer. 1991;67(10):2543–2551.
- Kassahun WT, Guenl B, Ungemach FR, et al. Expression and functional coupling of liver beta2 – adrenoceptors in the human hepatocellular carcinoma. Pharmacology. 2012;89(5–6):313–320.
- Chen D, Xing W, Hong J, et al. The beta2-adrenergic receptor is a potential prognostic biomarker for human hepatocellular carcinoma after curative resection. Ann Surg Oncol. 2012;19(11):3556–3565.
- Wang F, Liu H, Wang F, et al. Propranolol suppresses the proliferation and induces the apoptosis of liver cancer cells. Mol Med Rep. 2018;17(4):5213–5221.
- İşeri ÖD, Sahin FI, Terzi YK, et al. beta-Adrenoreceptor antagonists reduce cancer cell proliferation, invasion, and migration. Pharm Biol. 2014;52(11):1374–1381.
- Thiele M, Albillos A, Abazi R, et al. Non-selective beta-blockers may reduce risk of hepatocellular carcinoma: a meta-analysis of randomized trials. Liver Int. 2015;35(8):2009–2016.
- Yu D, Holmes S, Uhanova J, et al. Predicting hepatocellular carcinoma recurrence and survival. Hepatogastroenterology. 2014;61(131):776–783.
- Chang PY, Chung CH, Chang WC, et al. The effect of propranolol on the prognosis of hepatocellular carcinoma: a nationwide population-based study. PLOS One. 2019;14(5):e0216828.
- Barlow L, Westergren K, Holmberg L, et al. The completeness of the Swedish Cancer Register: a sample survey for year 1998. Acta Oncol. 2009;48(1):27–33.
- Wettermark B, Hammar N, MichaelFored C, et al. The new Swedish Prescribed Drug Register – opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidem Drug Safe. 2007;16(7):726–735.
- Weberpals J, Jansen L, van Herk-Sukel MPP, et al. Immortal time bias in pharmacoepidemiological studies on cancer patient survival: empirical illustration for beta-blocker use in four cancers with different prognosis. Eur J Epidemiol. 2017;32(11):1019–1031.
- Udumyan R, Montgomery S, Fang F, et al. Beta-blocker drug use and survival among patients with pancreatic adenocarcinoma. Cancer Res. 2017;77(13):3700–3707.
- Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11(1):450.
- Sjöberg H. Statistics Sweden. Swedish registers – a gold mine for medical research; 2016. http://epc2014.princeton.edu/papers/140708.
- Johansson LA, Westerling R. Comparing Swedish hospital discharge records with death certificates: implications for mortality statistics. Int J Epidemiol. 2000;29(3):495–502.
- Lambert PC, Royston P. Further development of flexible parametric models for survival analysis. The Stata Journal. 2009;9(2):265–290.
- Royston P, Sauerbrei W. Building multivariable regression models with continuous covariates in clinical epidemiology–with an emphasis on fractional polynomials. Methods Inf Med. 2005;44(04):561–571.
- Montomoli J, Erichsen R, Norgaard M, et al. Survival of patients with primary liver cancer in central and northern Denmark. Clin Epidemiol. 2011. 1998;3(2009):3–10.
- Mandorfer M, Reiberger T. Beta blockers and cirrhosis, 2016. Dig Liver Dis. 2017;49(1):3–10.
- Desai A, Sandhu S, Lai JP, et al. Hepatocellular carcinoma in non-cirrhotic liver: a comprehensive review. WJH. 2019;11(1):1–18.
- Garcia-Tsao G, Sanyal AJ, Grace ND, Practice Guidelines Committee of the American Association for the Study of Liver Diseases, the Practice Parameters Committee of the American College of Gastroenterology, et al. Prevention and management of gastroesophageal varices and variceal hemorrhage in cirrhosis. Hepatology. 2007;46(3):922–938.
- Giannelli V, Lattanzi B, Thalheimer U, et al. Beta-blockers in liver cirrhosis. Ann Gastroenterol. 2014;27(1):20–26.
- Senzolo M, Cholongitas E, Burra P, et al. beta-Blockers protect against spontaneous bacterial peritonitis in cirrhotic patients: a meta-analysis. Liver Int. 2009;29(8):1189–1193.
- Hernandez-Gea V, Aracil C, Colomo A, et al. Development of ascites in compensated cirrhosis with severe portal hypertension treated with beta-blockers. Am J Gastroenterol. 2012;107(3):418–427.
- Schutte K, Schulz C, Poranzke J, et al. Characterization and prognosis of patients with hepatocellular carcinoma (HCC) in the non-cirrhotic liver. BMC Gastroenterol. 2014;14(1):117.
- Zhang ZF, Feng XS, Chen H, et al. Prognostic significance of synergistic hexokinase-2 and beta2-adrenergic receptor expression in human hepatocelluar carcinoma after curative resection. BMC Gastroenterol. 2016;16(1):57.
- Cole SW, Nagaraja AS, Lutgendorf SK, et al. Sympathetic nervous system regulation of the tumour microenvironment. Nat Rev Cancer. 2015;15(9):563–572.
- Perez-Sayans M, Somoza-Martin JM, Barros-Angueira F, et al. Beta-adrenergic receptors in cancer: therapeutic implications. Oncol Res. 2010;19(1):45–54.
- Baker JG. The selectivity of beta-adrenoceptor antagonists at the human beta1, beta2 and beta3 adrenoceptors. Br J Pharmacol. 2005;144(3):317–322.
- Vandenbroucke J, Pearce N. Point: incident exposures, prevalent exposures, and causal inference: does limiting studies to persons who are followed from first exposure onward damage epidemiology? Am J Epidemiol. 2015;182(10):826–833.
- Fitzgerald PJ. Beta blockers, norepinephrine, and cancer: an epidemiological viewpoint. Clin Epidemiol. 2012;4:151–156.
- Danaei G, Tavakkoli M, Hernan MA. Bias in observational studies of prevalent users: lessons for comparative effectiveness research from a meta-analysis of statins. Am J Epidemiol. 2012;175(4):250–262.
- Grobbee DE, Hoes AW. Confounding and indication for treatment in evaluation of drug treatment for hypertension. BMJ. 1997;315(7116):1151–1154.
- Pinter M, Trauner M, Peck-Radosavljevic M, et al. Cancer and liver cirrhosis: implications on prognosis and management. ESMO Open. 2016;1(2):e000042.
- Moctezuma-Velazquez C, Kalainy S, Abraldes JG. Beta-blockers in patients with advanced liver disease: Has the dust settled? Liver Transpl. 2017;23(8):1058–1069.