
To the Editor,
We would like to thank Dr Green and Dr Kim for their kind interest in our article [Citation1], ‘Sudden cardiac death in the soccer field: a retrospective study in young soccer players from 2000 to 2013’ and to bring forth an important issue, such as the use of true denominators in the evaluation of SCD events, that we were able to document after a search of online databases. We would like to respond to their following comments:
They mention that the lack of a total denominator prevented us from calculating ‘a true incidence of SCD in this population’. However, the goal of our article was not to assess the incidence of SCD but rather to evaluate the surrounding or associated factors leading to SCD events as a hypothesis-generating approach to understand what triggers SCD at a specific time in athletes who, in most cases, have had an underlying congenital condition throughout their whole life and career [Citation2]. After completing our data gathering, we were able to document less events compared with previous reports [Citation3] published by members of the Fédération Internationale de Football Association Medical Assessment and Research Centre (F-MARC), by sending questionnaires to every Fédération Internationale de Football Association member association. Therefore, we did not attempt to calculate the incidence knowing that our database has fewer events that those reported by F-MARC, and would result in an underestimation of the problem.
Drs Green and Kim make a good point with their observation that the difference in events observed by each player position might be due to the relative percentage of players at each specific position, and we appreciate the time taken to conduct their search. In our discussion, this possibility could have been included as we did while discussing the observed distribution of events according to the athlete’s continent of origin. However, we realized that with their argument, they assume that every player of the squad is at the same risk at all times. This would be true if soccer was a game where all the members of the squad exercise a similar amount of time to the same level, as happens during training sessions. Vigorous physical activity can increase the risk of SCD in susceptible individuals [Citation4] and during matches, only 10 field players – and possibly 3 substitutions – of the whole squad can participate; with this, they would be at greater risk compared with their non-participating teammates.
Keeping this in mind, and that in our group almost 2/3 events occurred in players in matches rather than training, we decided to test their hypothesis even further. If the SCD frequency per position is a mere consequence of players distribution, we should not observe a difference of SCD events frequencies per position during matches, a setting in which measurements of covered distance and high-intensity running (we referred to in our article) were assessed [Citation5-7]. To this end, we decided to study the characteristics of those who collapsed during a match setting in the group we previously reported. We included those patients who collapsed during a match for whom their position was available (numerator). Events that occurred during training or more than 1 hour after physical activity were excluded. Goalkeepers were excluded from computation as no events were observed in this position during matches. In order to obtain the percentage of players per position during soccer matches (denominator), we conducted a search of 10 teams each of five different continental soccer federations (Union des associations européennes de football, Confederación Sudamericana de Fútbol, The Confederation of North, Central America and Caribbean Association Football, Confédération Africaine de Football and Asian Football Confederation). The top 10 teams from each federation in 2014 according to the International Federation of Football History and Statistics were selected as sample. For each team, the most common formation used in their last three games (as of 25 February 2015) was selected for analysis. Data regarding formation during each game and player’s position was collected on hierarchical order from: continental federation websites [Citation8-12], team’s website or electronic soccer database [Citation13,14]. Since we did not evaluate number of substitutions per position, we decided to exclude from our analysis those patients whose events occurred in a match, but who entered the game as substitutes. Data on formations and players from 47 out of 50 teams was available. The results are shown in and . This data reveals that defenders and midfielders represent a similar percentage of players in matches, and strikers about half of that. However, more events were evidenced in midfielders compared with defenders and strikers. After correcting the percentage of events of each position to the percentage of players per position, the midfielders suffered 1.7 times more events than defenders and 1.58 times more events than strikers (). Our goal with the article and the data is to prove that it might be worthwhile to investigate this trend even further, rather than assuming this observation is simply due to the number of players at risk. Especially because, there could be potential implications for preventive strategies, such as more thorough evaluations for players at greater risk.
Table 1. Number of field players during matches according to their position.
Figure 1. Comparison of sudden cardiac death events distribution according to player’s field position to distribution of field players during soccer matches in 47 worldwide teams.
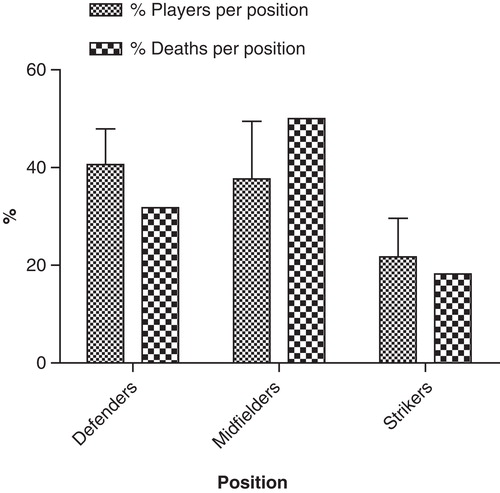
Table 2. Adjusted distribution of sudden cardiac death events during soccer matches according to player’s position.
Drs Green and Kim also argue that the fact of SCDs being observed in goalkeepers contradicts the hypothesis of high-intensity running. However, in our database more than half of the goalkeepers with SCD events suffered it during training, for which we have no way to estimate or prove they were not performing activity at similar intensity as other players, and not in actual matches during which they “… do not run extensively…” compared with field players.
Finally, our purpose was to bring up awareness that in the medical community little is known about the mechanism(s) that trigger SCD events in predisposed athletes. We are not arguing that our hypothesis is a proven fact, and we are aware of the several limitations of our approach, including the paucity of data and the impossibility to perform statistical analysis in the SCD group to confirm that our observations are not a consequence of hazard; unfortunately, the lack of large and high-quality databases make this approach the only one available to us so far. Hopefully, some questions will be answered with higher-quality databases, such as the sudden death registry and others with animal models of the underlying conditions that predispose for SCD in athletes.
Giovanni Davogustto, M.D.
John P. Higgins, M.D. MBA (Hons), MPHIL, FACC, FACP, FAHA, FACSM, FASNC, FSGC
Declaration of interest
The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties.
Notes
References
- Green G, Kim BY. Letter regarding sudden cardiac death in the soccer field. 2015; doi:10.1080/00913847.2015.1027639
- Corrado D, Pelliccia A, Bjornstad HH, Vanhees L, Biffi A, Borjesson M, et al. Study Group of Sport Cardiology of the Working Group of Cardiac R, Exercise P, the Working Group of M and Pericardial Diseases of the European Society of C. Cardiovascular pre-participation screening of young competitive athletes for prevention of sudden death: proposal for a common European protocol. Consensus Statement of the Study Group of Sport Cardiology of the Working Group of Cardiac Rehabilitation and Exercise Physiology and the Working Group of Myocardial and Pericardial Diseases of the European Society of Cardiology. Eur Heart J 2005;26:516–24
- Schmied C, Drezner J, Kramer E and Dvorak J. Cardiac events in football and strategies for first-responder treatment on the field. Br J Sports Med 2013;47:1175–8
- Thompson PD, Franklin BA, Balady GJ, Blair SN, Corrado D, Estes NAIII, Fulton JE, et al. Exercise and acute cardiovascular events placing the risks into perspective: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism and the Council on Clinical Cardiology. Circulation 2007;115:2358–68
- Andrzejewski M, Chmura J, Pluta B, Kasprzak A. Analysis of motor activities of professional soccer players. J Strength Cond Res 2012;26:1481–8
- Bradley PS, Sheldon W, Wooster B, Olsen P, Boanas P and Krustrup P. High-intensity running in English FA Premier League soccer matches. J Sports Sci 2009;27:159–68
- Di Salvo V, Gregson W, Atkinson G, Tordoff P and Drust B. Analysis of high intensity activity in Premier League soccer. Int J Sports Med 2009;30:205–12
- UEFA official Website. Available from http://www.uefa.com/
- CONCACAF Official Website. Available from http://www.concacaf.com/
- CONMEBOL Official Website. Available from http://conmebol.com/
- CAF official Website. Available from http://www.cafonline.com/
- AFC Official Website. Available from http://www.the-afc.com/
- ESPN Website. Available from http://espn.go.com/
- Soccerway. Available from http://us.soccerway.com/