
Sir
We read with interest Nagi et al.'s case report on an unusual presentation of incontinence due to vaginal entrapment of urine. We would like to share with the readers our experience of a similar case of urine entrapment secondary to detrusor overactivity.
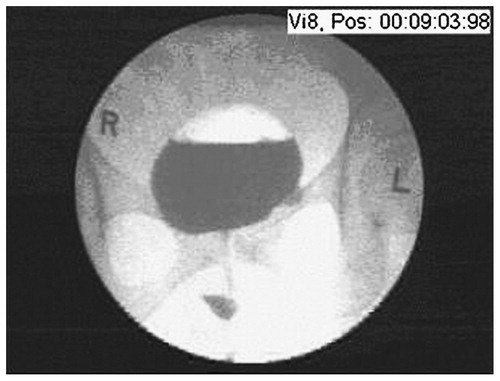
Mrs B.A. is a 42-year-old para 1 + 0 woman who had one caesarean section 9 years previously for failure-to-progress. She was referred with a 4 month history of continuous leakage per vaginam. This began after she started sexual activity following an abstinence of 4 years. She gave no recent history of surgery or trauma. The loss was not precipitated by increased intra-abdominal pressure and she denied any urge incontinence. Although she had longstanding frequency and urgency of micturition, the persistent loss of fluid was not associated with these symptoms. She sometimes complained of ‘vaginal laxity’ with intercourse and interestingly, she occasionally had coital incontinence associated with suprapubic cramps. On examination, copious watery loss was seen pooling in the posterior fornix but there was no demonstrable stress incontinence. Pelvic examination was unremarkable. High vaginal swab and chlamydial cultures were negative. Urinary fistula was unlikely in the absence of recent surgery and trauma but, in view of the unusual history and examination, a triple swab test with methylene blue was performed. We waited for over 1 h before examining the swabs, which remained only slightly damp and unstained. Intravenous pyelography was similarly negative. Hysteroscopy and cystoscopy revealed a normal uterine cavity and bladder, respectively. Laparoscopy showed moderate omental adhesions secondary to her previous caesarean section and these were lysed. Puzzled, we aspirated the fluid from the vagina and biochemical examination revealed a urea concentration of 86.6 mmol/l, suggesting the fluid was in fact urine and not vaginal discharge. Videocystourethrography was finally performed which demonstrated unstable bladder contractions in the filling phase and obvious trapping of urine in the vagina in the upright position (). It was likely that Mrs B.A. was unaware of the leakage that occurred due to detrusor overactivity, which then pooled in her vagina and gradually dribbled out. She was commenced on Tolteridone SR 4 mg and advised to alter the position in which she micturated in order to reduce the urine entrapment in the vagina. Her symptoms improved and she remains under review.
Figure 1. Entrapment of urine following detrusor contraction.
Reference
- Ben Nagi J, Robinson D, Cardozo L, Anders K. Anatomical entrapment – an unusual cause of urinary incontinence. Journal of Obstetrics and Gynaecology 2004; 24: 709–710