

Abstract
We carried out this study to validate the use of ultrasound sliding sign to predict intraperitoneal adhesions in women undergoing repeated caesarean section (CS). A cross-section study was performed in women with at least one CS scheduled for an elective CS. We used the sliding sign of the uterus against the anterior abdominal wall to assess intraperitoneal adhesions, positive sliding sign if uterus moved freely and a negative sliding sign if limited mobility. The obstetrician was blind to the ultrasound results, asked to report if adhesions were absent or present during CS to validate accuracy of the sliding sign. We examined 120 women, negative sliding was reported in 54 patients, positive sliding in 66 women. The presence of intra-abdominal adhesions was confirmed in 44/54 cases assigned to the high-risk group, while the prediction of low risk for adhesions confirmed in 66/66 patients with a sensitivity of 100%, specificity of 86.84%. Sliding sign is an effective method to detect intra-abdominal adhesions in women with a history of repeated caesarean delivery.
What is already known on this subject? There has been a dramatic increase in the caesarean section (CS) rate worldwide; repeated CSs may be associated with intraperitoneal adhesions that result in difficulty during the procedure and may be related to bowel or bladder injuries and neonatal morbidities.
What do the results of this study add? The sliding sign by ultrasound has a sensitivity of 100%, specificity of 86.84%, a positive predictive value of 81.5, a negative predictive value of 100, and accuracy of 91.67, considering it rapid, easy and reliable method for prediction of intraperitoneal adhesions.
What are the implications of these findings for clinical practice and/or future research? The use of sliding sign by ultrasound in cases with repeated CSs offers a good predictor tool for presence of intraperitoneal adhesions and subsequently avoid severe sequels during surgery and good preparation.
Impact statement
Introduction
Caesarean section (CS) is a procedure that involves the extraction of the baby from the mother's abdomen for numerous foetal and maternal indications. The CS rate has increased dramatically in the last decade, reaching up to 32% in the USA (2014) and 38% (2011) at Assiut University in Egypt (Abdel-Aleem et al. Citation2013; Betrán et al. Citation2016).
Caesarean section is associated with many intra- and postoperative complications. Early complications include haemorrhage, bladder and bowel injuries, sepsis and postoperative ileus (Field and Haloob Citation2016). Remote complications include the occurrence of intraperitoneal adhesions. The incidence of adhesions varies according to many factors, including the number of previous CSs, type of suture material, and haemostasis. Moreover, the incidence of adhesions after caesarean is between 12 and 75% (Berghella et al. Citation2013).
The presence of adhesions in repeated CSs increases surgical difficulties and the incidence of bladder and bowel injuries (Van Der Krabben et al. Citation2002; Rahman et al. Citation2009). A multidisciplinary team should properly evaluate these patients before surgery. Few studies used ultrasound to evaluate the presence of adhesions before operation (Ayachi et al. Citation2018; Baron et al. Citation2018). However, they either used transvaginal ultrasound that may not be available or used a small sample size that does not accurately reflect the value of this tool. A novel technique was first described by Baron et al. (Citation2018) using the dynamic ultrasound sliding sign to predict presence of intraperitoneal adhesions in women with a repeated section.
Materials and methods
This study was a blinded cross-section study where the investigator performed the ultrasound on the recruited participants before their elective CS to detect positive and negative sliding sign, and then the obstetrician (who was blinded to the ultrasound results) was informed to fill a postoperative report about presence or absence of moderate or severe intraperitoneal adhesions.
Study settings and durations
This study was carried out in Assiut University Hospital (tertiary hospital) and El-Eman Specialized Hospital of Obstetrics and Gynecology, Assiut Governorate, Egypt, between February 2019 and February 2020.
All pregnant women who attended the hospitals mentioned above in their third trimester of pregnancy and needed an elective repeated CS (who were not in labour at the time of attendance) were eligible for this study. The Assiut University Faculty of Medicine Ethical Review Board approved the study.
Inclusion criteria were an age between 18 and 45 years; pregnant women in their third trimester who planned to undergo an elective CS with a history of at least one previous CS and accepted to participate in this study.
Exclusion criteria included women who planned their primary elective CSs; women who underwent an unplanned repeat caesarean delivery because of urgency (they might not have undergone complete preoperative assessment). Furthermore, women with known connective tissue/collagen disease and women with other previous surgery rather than CS were excluded.
Eligible women were subjected to preliminary evaluation, including history taking, clinical examination, body mass index (BMI) assessment and ultrasound examination to ensure the integrity of the pregnancy.
Intervention
All pregnant women planned to do an elective CS underwent a preoperative trans-abdominal ultrasound examination in the supine position by two examiners, senior resident (level I sonographer) and the specialist (level II sonographer). All of the examinations were performed using Medison ultrasound machine 5 MHz abdominal convex probe.
The probe was placed perpendicular just above the site of the previous caesarean incision then moved from above downward and from side to side, and we asked the patient to breathe deeply. Then, we recorded the movement of the anterior uterine wall against the anterior abdominal wall where positive sliding sign if the uterus moved freely indicates no adhesions and negative sliding sign if there was limited mobility (Baron et al. Citation2018). Subsequently, another experienced sonographer, blinded to patient data, independently viewed the video recordings, and classified a positive sliding sign if the anterior uterine wall was sliding across the abdominal wall and a negative sliding sign when there was no such relative motion.
Then, an elective caesarean was performed by the obstetrician on duty as scheduled, who was blind to the ultrasound results, and then we asked him to report if adhesions were absent or present. The presence of moderate or severe adhesions was defined as adhesions that cause a very difficult uterine access or the presence of bowel or bladder adhesions to the anterior side of the uterus complicating uterine access. Other findings were classified as no adhesions: we excluded mild and filmy adhesions.
Statistical methods
All statistical calculations were carried out using SPSS (Statistical Package for the Social Sciences; SPSS Inc., Chicago, IL) version 22. Data were statistically described in terms of mean±standard deviation (±SD), or median and range when not normally distributed, frequencies (number of cases) and relative frequencies (percentages) when appropriate. For comparing categorical data, Chi-square (χ2) test was performed. Receiver operating characteristic (ROC) curve analysis was done; p value was always two tailed set significant at .05 level.
Sample size calculation
Calculation of sample size was conducted using ‘statistics and sample size pro’ MS Excel Sample Size Calculator for Diagnostic Test Studies. According to the following inputs: expected sensitivity = 76.0%, expected specificity = 92.0%, expected prevalence of CS (CS rate at our centre) = 38.0% (Abdel-Aleem et al. Citation2013), desired precision = 12.0%, confidence interval = 95%. The sample size was 129 subjects.
Results
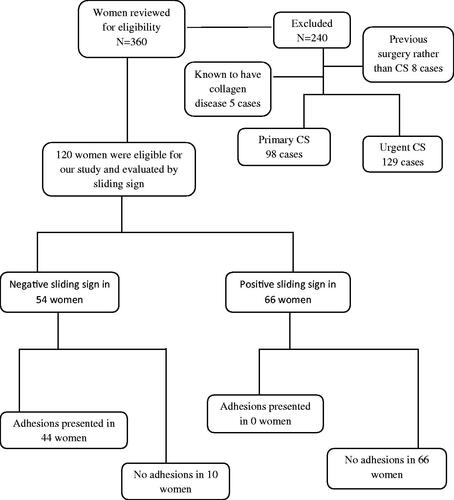
We recruited 360 women, and 240 were excluded; 102 had a primary CS while 138 were urgent cases, five were known to have collagen disease, and eight had previous surgery rather than CS, so we examined 120 women for sliding sign before their elective CS ().
Figure 1. Study flowchart.
The mean maternal age at our study was 26.70 ± 5.01 years and ranged from 20 to 40 years, mean parity was 2.49 ± 1.12 and ranged from 1 to 5. As regards to the number of previous CS, 43 of the women (36%) had undergone only one previous CS, 36 (30%) had two, 28 (23%) had three and 13 (11%) had more than or equal to four previous CS deliveries as regards the place of delivery 57 (47%) delivered at a governmental place and 63 (53%) delivered at a private place. For the gestational age at the time of delivery, 100 of neonates were full term at the time of delivery (83% were ≥37 weeks) and 20 (17%) were preterm (33–36 weeks). These cases of preterm deliveries were for cases with medical disorders; preeclampsia, and uncontrolled diabetes mellitus, that indicated caesarean delivery. The mean BMI of studied women at the time of delivery (kg/m2) was 29.37 ± 4.24 and ranged from 19.8 to 44.4 kg/m2, 18 (15%) had normal BMI, 49 (41%) were overweight and 53 (44%) were obese ().
Table 1. Demographic characteristics of study women who undergoing repeat a caesarean section (n = 120).
shows that there were statistically significant associations between the presences or absences of intra-operative adhesions and maternal age groups (years), where women with age ≥30 years old have a higher incidence of adhesions than women with younger age (p = .001); the number of previous parity, where women with higher parity ≥3 has a higher incidence of adhesions than women with lower parity (p = .001); the number of previous CS, with increased number of previous CS there is an increase in the incidence of adhesions (p = .001); gestational age (weeks), where term delivers associated with a higher incidence of adhesions (p = .004); and BMI (kg/m2), where obese women have a higher incidence of adhesions (p = .004).
Table 2. Associations between different demographic and clinical data and intra-abdominal adhesions in women with repeat caesarean delivery (n = 120).
Examination of the sliding sign was performed successfully in 120 women. Negative sliding of the uterus was noted in 54 patients, whereas positive sliding was present in 66 women. The suspicion of the presence of moderate or severe intra-abdominal adhesions was confirmed at the surgery in 44 of the 54 cases assigned to the high-risk group, prevalence of moderate or severe adhesions was 36.6% (44/120), whilst the prediction of low risk for adhesions was confirmed in 66 of 66 patients ().
Table 3. Diagnosis of intra-abdominal adhesions based on sliding sign on trans-abdominal ultrasound and findings during caesarean section (CS), in 120 women undergoing repeated CS.
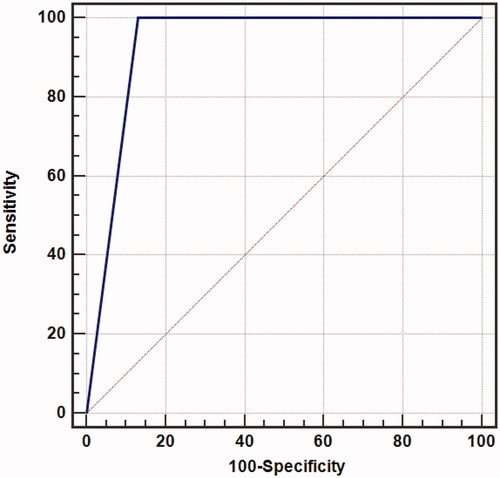
shows the predictive ability of the sliding sign for the detection of intra-abdominal adhesions in women with repeat caesarean delivery using the ROC curve analysis. The area under the ROC curves for sliding sign was 0.934. Sensitivity of 100% (95% CI 92–100), specificity of 86.84% (95% CI 77.1–93.5), PPV of 81.5% (95% CI 68.6–90.7), NPV of 100% (95% CI 96.6–100) with overall accuracy 91.67%, (p = .001). Sliding sign was observed to be a significantly better predictor for the detection of intra-abdominal adhesions in women with repeat caesarean delivery (p = .001).
Figure 2. ROC.
Discussion
The CS rate is currently increasing dramatically, leading to increased complications such as placenta accreta spectrum and intraperitoneal adhesions, which may show on some occasions to significant difficulties during CS with a negative impact on the mother and the neonate. The present study was a prospective observational study aimed at validating dynamic ultrasound to predict intra-abdominal adhesions in women undergoing repeated CSs. The study included 120 pregnant women who planned to undergo elective CS with a history of at least one previous CS.
While reviewing the literature for methods for prediction of intraperitoneal adhesions during repeated CS, four studies were concerned about the evaluation of the accuracy of the dynamic ultrasound by the sliding sign for prediction of intraperitoneal adhesions in women with repeated CSs, the first one by Baron et al. (Citation2018), who examined 63 women by the novel technique the sliding sign for detection of intraperitoneal adhesions, the second by Drukker et al. (Citation2018) with larger sample size 370 women, the third one by Bukar et al. (Citation2022) and the last one by Shu (Citation2021). Other studies used different parameters to predict intraperitoneal adhesions like CS wound scar characters, and the index for intraperitoneal adhesions was out of our scope (Pergialiotis et al. Citation2017).
The mean maternal age of our study participants was 26.70 ± 5.01 years which was lower than the mean age reported by Baron et al. (Citation2018) and Drukker et al. (Citation2018), which was 34.6 ± 1.15 and 34.465.1 years, respectively, the early age of marriage at our community can explain that. Our results showed that the mean parity was 2.49 ± 1.12, which was quite similar to Bukar et al. (Citation2022), who reported mean parity as 2.42 ± 1.17.
As regards to the number of previous CS, 43 women (36%) had undergone only one previous CS, 36 (30%) had two, and 41 (34%) more than two previous CS deliveries. Our results are in agreement with a prior study by Drukker et al. (Citation2018) who reported that 112 (30%) had undergone only one previous CS, 135 (37%) had two and 123 (33%) had three or more previous CS deliveries. On the other hand, Baron et al. (Citation2018) reported a higher rate of CSs, eight (13%) had undergone only one previous CS, 20 (34%) had two and 31 (53%) more than two previous CS deliveries and this can be explained by higher mean parity reported by Baron et al. (Citation2018). In our study, 44.2% of women were obese, with a mean BMI of 29.37 ± 4.24 kg/m2, which was quite similar to the BMI study which was 30.96 ± 5.5 kg/m2 (Drukker et al. Citation2018).
The prevalence of moderate and severe adhesions among our study participants was 36.6% (44 patients out of 120 confirmed intraoperative to have severe or moderate adhesions during CS) comparable to findings by Baron et al. (Citation2018) and by Bukar et al. (Citation2022); 35.5 and 33.8%, respectively, and higher than the prevalence reported by Shu (Citation2021) at 13.4%. This could be explained by the difference in the number of previous CS in a study by Shu et al. most cases, 90.1%, had only previous CS.
We reported a statistically significant association between the presences or absences of intra-operative adhesions and maternal age groups (years), where women with age ≥30 years old have a higher incidence of adhesions than women with younger age (p = .004). This can be explained by higher parity with increased age and higher number of CS. Regards the number of parity, women with higher parity ≥3 have a higher incidence of adhesions compared to women with lower parity (p = .001); with repeated CS, the incidence of adhesions increased significantly (p = .001); gestational age (weeks), where preterm (33–36 weeks) deliveries associated with a higher incidence of adhesions (p = .002); and BMI (kg/m2), where obese women have a higher incidence of adhesions (p = .001). Unfortunately, no previous publications address the same associations.
Negative sliding of the uterus was reported in 54 patients, whereas positive sliding was present in 66 women. The suspicion of intra-abdominal adhesions was confirmed at the surgery in 44/54 cases assigned to the high-risk group (women with negative sliding sign), while the prediction of low risk for adhesions was confirmed in 66 of 66 women, and by measuring the predictive ability to slide sign for the detection of intra-abdominal adhesions in women with repeat caesarean delivery using the ROC curve analysis. We analysed that the area under the ROC curves was 86.9, the sensitivity of 100%, specificity of 86.84% with overall accuracy 85%.
Our results agreed with results by Bukar et al. (Citation2022), who reported sensitivity and specificity of 100% of the sliding sign for detection of intraperitoneal adhesions and results by Baron et al. (Citation2018), who reported sensitivity of 76.2% and a specificity of 92.1%. In contrast, Drukker et al. (Citation2018) and Shu (Citation2021) reported lower sensitivity 56 and 53.3%, respectively.
The strength of our study includes its novelty and blinded-prospective design. Our study is the first Egyptian study to assess the role of trans-abdominal ultrasound in predicting adhesions in women with repeated CSs. The main limitations were the small sample size and the presence of different surgeons performing CS, which affect the judgement of the severity of adhesions.
Conclusions
We conclude that applying a preoperative TAU to detect severe intra-abdominal adhesions has the advantage of simplicity. Predicting severe adhesions based on a negative sliding sign can result in better planning and safer conduction of surgery. Furthermore, improved perioperative decision-making process concerning the timing of surgery, surgeon seniority, anaesthetic team, type of anaesthesia, surgical technique, preparation of blood products, and the high level of care is required in women suspected of having intra-abdominal adhesions.
Author contributions
AY, AAY and AA contributed in this work by designing the study and writing the initial draft. SM, AM and MI contributed equally to this work by data acquisition, analysis and final editing. AY and MI contributed in the study conception, design and supervision. All authors read and approved the final manuscript.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Abdel-Aleem H, Shaaban OM, Hassanin AI, Ibraheem AA. 2013. Analysis of cesarean delivery at Assiut University Hospital using the Ten-Group Classification System. International Journal of Gynecology & Obstetrics 123:119–123.
- Ayachi A, Bouchahda R, Derouich S, Mkaouer L, Kehila M, Abouda H, et al. 2018. Accuracy of preoperative real‐time dynamic transvaginal ultrasound sliding sign in prediction of pelvic adhesions in women with previous abdominopelvic surgery: prospective, multicenter, double‐blind study. Ultrasound in Obstetrics & Gynecology 51:253–258.
- Baron J, Tirosh D, Mastrolia SA, Ben-Haroush Y, Schwartz S, Kerner Y, et al. 2018. Sliding sign in third-trimester sonographic evaluation of intra-abdominal adhesions in women undergoing repeat cesarean section: a novel technique. Ultrasound in Obstetrics & Gynecology 52:662–665.
- Berghella V, Lockwood C, Barss V. 2013. Cesarean delivery: postoperative issues. Waltham: UpToDate.
- Betrán AP, Ye J, Moller A-B, Zhang J, Gülmezoglu AM, Torloni MR. 2016. The increasing trend in caesarean section rates: global, regional and national estimates: 1990–2014. PLOS One 11:e0148343.
- Bukar M, Mana AU, Ikunaiye N. 2022. Preoperative sonographic prediction of intra-abdominal Adhesions using sliding sign at repeat caesarean section at the University of Maiduguri Teaching Hospital, Nigeria: a prospective observational study. BMJ Open 12:e046334.
- Drukker L, Sela HY, Reichman O, Rabinowitz R, Samueloff A, Shen O, et al. 2018. Sliding sign for intra-abdominal adhesion prediction before repeat cesarean delivery. Obstetrics and Gynecology 131:529–533.
- Field A, Haloob R. 2016. Complications of caesarean section. Obstetrician & Gynaecologist 18:265–272.
- Pergialiotis V, Frountzas M, Siotos C, Karampetsou N, Perrea DN, Efthymios Vlachos D. 2017. Cesarean wound scar characteristics for the prediction of pelvic adhesions: a meta-analysis of observational studies. Journal of Maternal-Fetal & Neonatal Medicine 30:486–491.
- Rahman M, Gasem T, Al Suleiman S, Al Jama FE, Burshaid S, Rahman J. 2009. Bladder injuries during cesarean section in a University Hospital: a 25-year review. Archives of Gynecology and Obstetrics 279:349–352.
- Shu W. 2021. Predicting intra-abdominal adhesions for repeat cesarean delivery with the ultrasound sliding sign. Journal of Obstetrics and Gynaecology Canada 43:1274–1278.
- Van Der Krabben A, Dijkstra F, Nieuwenhuijzen M, Reijnen M, Schaapveld M, Van Goor H. 2002. Morbidity and mortality of inadvertent enterotomy during adhesiotomy. British Journal of Surgery 87:467–471.