

Abstract
This study aimed to evaluate physical and intellectual development of one-year-old infants of monochorionic twins with selective intrauterine growth restriction (sIUGR). A total of 31 pairs of sIUGR twins ageing 1 year old were included in the study. Each pair of sIUGR twins was divided into low birthweight-twin group (L-twin group) and high birthweight-twin group (H-twin group) according to twins’ birthweight. The differences in height, weight, head circumstance and body mass index (BMI) in each stage were statistically significant for all measures from birth until 1 year old (p < .05), and there was a disappointed catch-up growth in lighter twins. Psychomotor development index (PDI) and mental development index (MDI) at 1 year old were significantly different between the two groups (p < .05). Stepwise regression analysis showed that the effects of weight on both PDI and MDI were statistically significant (p < .05). Intrauterine growth inconsistencies in monochorionic twins with sIUGR persist until the first year of life and affect low-birthweight infants’ physical and intellectual development.
What is already known on this subject? Selective intrauterine growth restriction in monochorionic twins increases the risks of intrauterine foetal demise, preterm birth, caesarean delivery and adverse neonatal outcomes, especially in the smaller foetus.
What do the results of this study add? Previous studies have concentrated on the clinical management of sIUGR, while little attention has been paid to the growth and development of twins after birth. Given the adverse neurobiological effects of suboptimal nutrition on the brain development, it is important to determine whether IUGR causes long-term cognitive deficits and physical retardation. The current study has assessed the physical and intellectual development of one-year-old infants of monochorionic twins with sIUGR.
What are the implications of these findings for clinical practice and/or further research? Intrauterine growth inconsistencies in monochorionic twins with sIUGR persist until the first year of life and affect low-birthweight infants’ physical and intellectual development. Further research on the longer-term effects of sIUGR is needed.
Impact Statement
Introduction
Selective intrauterine growth restriction (sIUGR) could complicate 10–15% of monochorionic (MC) twin pregnancies (Lewi et al. Citation2008; Bennasar et al. Citation2017), and it was defined as an intertwin estimated foetal weight (EFW) discordance over 25% with one twin having an EFW below the 10th percentile (Valsky et al. Citation2010; Khalil et al. Citation2016). This pathology could increase the risk of intrauterine foetal death, preterm birth, caesarean delivery and adverse neonatal outcomes, especially in smaller foetuses (Khalil and Thilaganathan Citation2019). To date, studies have concentrated on clinical management of sIUGR, while little attention has been paid to the growth and development of twins after birth. It is well-known that the prenatal period is a time of rapid brain development, which includes remarkable changes in cortical folding (Battin et al. Citation1998), myelination (Counsell et al. Citation2002) and grey-matter distribution (Isaacs et al. Citation2001). These findings raise the hypothesis that infants who suffer from growth restriction during the prenatal period are likely to be deprived of an optimal supply of nutritional substrates, and they are at risk of impaired neural and cognitive development. Given the adverse neurobiological effects of suboptimal nutrition on the brain development, it is essential to determine whether IUGR causes long-term cognitive deficits and physical retardation. The current study has assessed the physical and intellectual development of one-year-old infants of MC twins with sIUGR.
Methods
Subjects
A total of 62 consecutive infants consisting of 31 pairs of one-year-old sIUGR twins, who were admitted to the Neonatal Neurodevelopmental Clinic at the Second Affiliated Hospital of Wenzhou Medical University (Wenzhou, China), were enrolled in this study. The study was approved by the Institutional Review Board of the Second Affiliated Hospital of Wenzhou Medical University (approval no. LCKY2019-288). All the subjects’ parents signed the informed consent form. The exclusion criteria included major congenital anomalies, known congenital syndromes, or significant ongoing illnesses, such as short bowel syndrome or bronchopulmonary dysplasia.
Procedure
Monochorionicity was clarified on the first-trimester ultrasound and chorionic examination after delivery. MC twins whose birth weights differed by over 25% with one twin having a birth weight below the 10th percentile were classified as sIUGR. In addition to birth weight, birth length, head circumference at birth, body mass index (BMI), gestational age (GA), complication with velamentous cord insertion, parents’ occupation, educational levels, and method of conception (in vitro fertilisation (IVF), use of clomid, or spontaneous) were recorded. Perinatal outcome was assessed according to the 1-min and 5-min Apgar scores, admission to a newborn intensive care unit (NICU), length of stay, and neonatal hypoglycaemia.
Each pair of sIUGR twins was divided into low birthweight-twin group (L-twin group) and high birthweight-twin group (H-twin group) according to twins’ birthweight. The height, weight and head circumference of each child were measured at birth, 1 month old, 3 months old, 6 months old, 8 months old and 1 year old. Circling the posterior occipital tuberosity through the upper part of the arched eyebrow was used for the measurement of head circumference.
Bayley scales of infant development (BISD), including intelligence scale and exercise scale, were used to test infants’ psychomotor and mental development. The intelligence scale and exercise scale were expressed by the mental development index (MDI) and psychomotor development index (PDI), respectively. After obtaining full familiarity and cooperation from the infants in a quiet environment, the evaluation process was carried out item by item to figure out the MDI and PDI. The evaluation was repeated after 15 days without satisfying cooperation. Cognitive performance tests were performed by expert psychologists who were unaware of twins’ status at the Institute of Cognitive Sciences of the Second Affiliated Hospital of Wenzhou Medical University.
Statistical analysis
The smooth spline function of R 3.5.3 software (R Foundation for Statistical Computing, Vienna, Austria) was used to fit the sample data with three smoothing splines. First, the parameter ‘CV = true’ was set to select the appropriate degree of freedom for the group with a small sample size using the leave-one-out cross-validation. Then, the fitting curves of the physical indicators in each group were drawn based on the degree of freedom. SPSS 26.0 software (IBM Corp., Armonk, NY) was used to perform the statistical analysis. The paired t-test was used to compare the measurement data among groups for normally distributed data, which were expressed as mean ± standard deviation (x ± s), while the Wilcoxon rank-sum test was used to compare abnormally distributed data, which were expressed as (minimum, maximum). The χ2 test was used for comparing counting data, which were expressed as ratio or constituent ratio. In univariate analysis, the t-test was used to compare normally distributed variables among groups, the Mann–Whitney U-test was utilised for comparing skewed distributed variables, and Fisher’s exact test was used for comparing classified variables. In multivariate analysis, linear regression analysis was used. p < .05 was considered statistically significant.
Results
Subjects’ basic data
During the study period, 40 pairs of MC twins who had a birth weight discordance of ≥25% were enrolled. It is noteworthy that six families had left the city and three families did not consent to participate in the study. Thus, a total of 31 pairs (inclusion rate, 77%) of MC twins (14 male and 17 female pairs) were finally included. Mean GA at birth was 35 (33–35) weeks, the average age of pregnant women was 28 (range, 25–31) years old. The average birth weight in the L-twin group was 1693 (range, 880–2280) g, and it was 2394 (range, 1520–3300) g in the H-twin group. The mean birth weight difference was 699 (range, 470–1020) g, and the EFW was 29.72% (range, 25–46%). Among 31 pairs of twins, there were 18, 2 and 11 cases of sIUGR I, II and III types, respectively. Besides, 80.6% of cases underwent emergency caesarean section to terminate the pregnancy.
As shown in , length, weight, head circumstance and BMI were lower in the L-twin group compared with those in the H-twin group (p < .05). The prevalence of velamentous placenta and average length of stay were higher in the L-twin group than those in the H-twin group (p < .05). There was no statistically significant difference in the rate of admission to the NICU, neonatal hypoglycaemia or Apgar scores between the two groups.
Table 1. Compare the characteristics of sIUGR at birth.
Physical development
The physical growth data of 31 pairs of sIUGR twins at birth, 1 month old, 3 months old, 6 months old, 8 months old and 1 year old were reviewed, and the fitting curves of body weight, height, head circumference and BMI were respectively drawn (). The height, weight, head circumference and BMI in the L-twin group were significantly lower than those in the H-twin group at all months within 1 year old (p < .05). As shown in , the rate of physical growth at 3 months old, 6 months old, 8 months old and 1 year old in the L-twin group was significantly higher than that in the H-twin group (p < .05); however, ultimately, the L-twin group did not surpass the H-twin group in terms of height, weight and head circumference at 1 year old.
Figure 1. The physical growth data of 31 pairs of sIUGR twins.
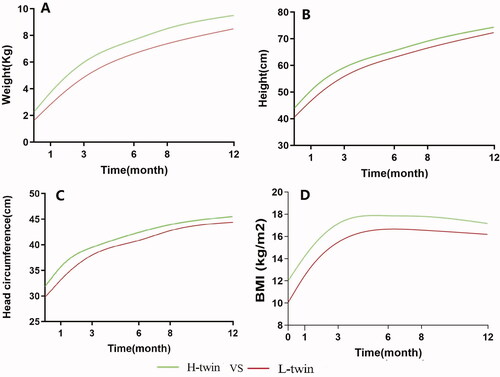
Table 2. The rate of physical growth data of two groups.
Evaluation of PDI and MDI
It was found that the PDI and MDI at 1 year old in the L-twin group were significantly lower than those in the H-twin group (p < .05) (). There was no significant difference in PDI and MDI between sIUGR I and sIUGR III at 1 year old (p > .05).
Table 3. Bayley scales assessment results for L-twin vs. H-twin.
In addition, MDI and PDI were analysed in 62 cases by the multiple linear regression. PDI and MDI were taken as dependent variables, and weight, height, head circumference, the type of sIUGR, GA, sex, asphyxia (Apgar score≤ 7), neonatal hypoglycaemia, velamentous placenta and IVF were taken as independent variables. It was found that the effects of weight on PDI {β = 0.031 (95% CI: 0.013–0.049), p < .001} and MDI {β = 0.023 (95% CI: 0.003–0.043), p < .05} were statistically significant. The stepwise regression analysis indicated that the effects of weight on both PDI and MDI were statistically significant (p < .05).
Discussion
It is noteworthy that sIUGR is a severe complication of MC twin pregnancies, which is characterised by a large inter-twin growth discrepancy. Obstetricians need to declare amniotic and chorionic sex on ultrasound during the first trimester of twin pregnancies to provide a basis for further treatment. Several studies examined the perinatal outcomes of MC twin pregnancies complicated by sIUGR, and high rates of foetal demise (16–29%) and neonatal morbidities, such as cerebral injury (0–33%) were reported, depending on the umbilical artery Doppler classification (Inklaar et al. Citation2014; Arınkan et al. Citation2019). Whereas, there persists a glaring research gap that is of great importance to clinicians and families. For parents, the most important concern is the health and quality of life of their child or children after survival (Morris et al. Citation2015), and it has not yet been comprehensively assessed in the long-term results of multiple pregnancy studies (Groene et al. Citation2019).
To date, few researches have concentrated on physical and intellectual development after the birth of twins with sIUGR, and even for discordant twins, data describing growth patterns are also limited. Mazkereth et al. (Citation2014) studied on growth parameters (weight, length and head circumference) of discordant preterm twins during their first year of life, and found that the gaps in growth parameters between the smaller twins of preterm discordant twins and their larger siblings were significantly reduced, which were similar to the results of the present study on twins with sIUGR. The difference in height, weight, head circumstance and BMI in each stage were statistically significant in twins with sIUGR from their birth until the age of 1 year old, although there was a disappointed catch-up growth in lighter twins. Ross et al. (Citation2012) suggested that smaller discordant birth weight twins performed significantly less well on intelligence, although they did not significantly differ from their larger twins on growth parameters at 3 years old. Several studies confirmed that twins attained a normal final physical development compared with children from the general population until late adolescence (Van Dommelen et al. Citation2008; Estourgie-van Burk et al. Citation2010). We may follow-up these twins with sIUGR to indicate whether there would be a gap in physical parameters at any stage.
IUGR in critical periods of brain development may deprive the nutritional contents in the brain required for normal growth and development (Morgane et al. Citation1993). In the cohorts on MC twins, some scholars (Edmonds et al. Citation2010; Torche and Echevarría Citation2011; Murray et al. Citation2015) reported foetal growth restriction (FGR) results in lower neurocognitive scores in early childhood, and there remained significant differences in size, while others presented opposite findings (Reolon et al. Citation2008; Frezza et al. Citation2011).
However, these studies did not rule out the effects of twin-to-twin transfusion syndrome (TTTS), causing a very poor prognosis in newborns. In the present study, monozygotic twins with sIUGR were enrolled to reduce the effects of confounding factors. The results showed that the PDI and MDI at 1 year old in the L-twin group were significantly lower than those in the H-twin group. The results of the stepwise regression analysis revealed that weight has a significant effect on both PDI and MDI. Our results are similar to those reported by Swamy et al. who demonstrated that the FGR resulted in lower neurocognitive scores in early childhood, and there were significant differences in size (Swamy et al. Citation2018). Several studies have shown a strong association of low birth weight with adults’ growth and health (Barker and Hanson Citation2004). Furthermore, our results suggested that suboptimal intrauterine growth was related to impaired cognitive outcomes, and the reduced birth weight could be a risk factor for cognitive outcomes. Obstetricians are asked to pay close attention to the long-term cognitive effects of FGR and low birth weight infants.
MC twins reduce biases caused by confounding factors, such as genetics, intrauterine nutrition, maternal age and medication use. However, our study has also several limitations. The assessment was performed during 1 year old, and small sample size was noteworthy. The majority of developmental problems in children who were born very preterm can be identified in early childhood through regular follow-up (Jois Citation2019). Further research on the longer-term effects of sIUGR is needed. Although the assessment of both twins was performed simultaneously, it remains elusive whether the differences may persist into childhood, adolescence and later life.
Birth weight can be considered as an index of foetal nutrition, and it is influenced by maternal factors and prenatal genetics (Horikoshi et al. Citation2013, Citation2016), in which the latter acts through the intrauterine environment. Recent and novel evidence suggested that in particular altered expression of selective miRNA may play a key role in FGR (Chiofalo et al. Citation2017). Hence, it is essential to indicate which biomarkers (Laganà et al. Citation2017; Amodeo et al. Citation2022) are associated with the progression of FGR, especially sIUGR, and they can be necessary to improve early diagnosis and treatment of the disease. Recent evidence suggested that appropriate cofounders may be social environment and postnatal interventions in addition to biological factors, with particular attention paid to potentially modifiable factors in an effort to identify areas for future intervention efforts (Bills et al. Citation2021).
In summary, intrauterine growth inconsistencies in MC twins with sIUGR persist until the first year of life and affect low-birthweight infants’ physical and intellectual development. Concentration on specific interventions to boost the physical and intellectual development of growth-restricted children may be worthy of consideration. Further research on the longer-term effects of sIUGR is required.
Acknowledgements
We are grateful to children and their parents who participated in this study.
Disclosure statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Additional information
Funding
References
- Amodeo S, Cavoretto P, Seidenari A, Paci G, Germano C, Monari F, et al. 2022. Second trimester uterine arteries pulsatility index is a function of placental pathology and provides insights on stillbirth aetiology: a multicenter matched case-control study. Placenta 121:7–13.
- Arınkan S, Arısoy R, Api M. 2019. Assessment of pregnancy outcomes among twin pregnancies with single fetal demise regarding chorionicity and fetal death time. Journal of the Turkish German Gynecological Association 20:147–153.
- Barker D, Hanson M. 2004. Altered regional blood flow in the fetus: the origins of cardiovascular disease? Acta Paediatrica 93:1559–1560.
- Battin MR, Maalouf EF, Counsell SJ, DCR B, Herlihy AH, Rutherford MA, et al. 1998. Magnetic resonance imaging of the brain in very preterm infants: visualization of the germinal matrix, early myelination, and cortical folding. Pediatrics 101:957–962.
- Bennasar M, Eixarch E, Martinez J, Gratacós E. 2017. Selective intrauterine growth restriction in monochorionic diamniotic twin pregnancies. Seminars in Fetal & Neonatal Medicine 22:376–382.
- Bills S, Johnston J, Shi D, Bradshaw J. 2021. [Formula: see text] Social-environmental moderators of neurodevelopmental outcomes in youth born preterm: a systematic review. Child Neuropsychology 27:351–370.
- Chiofalo B, Laganà A, Vaiarelli A, La Rosa V, Rossetti D, Palmara V, et al. 2017. Do miRNAs play a role in fetal growth restriction? A fresh look to a busy corner. BioMed Research International 2017:6073167.
- Counsell S, Maalouf E, Fletcher A, Duggan P, Battin M, Lewis H, et al. 2002. MR imaging assessment of myelination in the very preterm brain. American Journal of Neuroradiology 23:872–881.
- Edmonds C, Isaacs E, Cole T, Rogers M, Lanigan J, Singhal A, et al. 2010. The effect of intrauterine growth on verbal IQ scores in childhood: a study of monozygotic twins. Pediatrics 126:e1095–101.
- Estourgie-Van Burk G, Bartels M, Boomsma D, Delemarre-Van De Waal H. 2010. Body size of twins compared with siblings and the general population: from birth to late adolescence. Journal of Pediatrics 156:586–591.
- Frezza S, Gallini F, Puopolo M, De Carolis M, D'Andrea V, Guidone P, et al. 2011. Is growth-discordance in twins a substantial risk factor in adverse neonatal outcomes? Twin Research and Human Genetics 14:463–467.
- Groene SG, Tollenaar LSA, Oepkes D, Lopriore E, Van Klink JMM. 2019. The impact of selective fetal growth restriction or birth weight discordance on long-term neurodevelopment in monochorionic twins: a systematic literature review. Journal of Clinical Medicine 8:944.
- Horikoshi M, Beaumont R, Day F, Warrington N, Kooijman M, Fernandez-Tajes J, et al. 2016. Genome-wide associations for birth weight and correlations with adult disease. Nature 538:248–252.
- Horikoshi M, Yaghootkar H, Mook-Kanamori D, Sovio U, Taal H, Hennig B, et al. 2013. New loci associated with birth weight identify genetic links between intrauterine growth and adult height and metabolism. Nature Genetics 45:76–82.
- Inklaar MJ, Van Klink JM, Stolk TT, Van Zwet EW, Oepkes D, Lopriore E. 2014. Cerebral injury in monochorionic twins with selective intrauterine growth restriction: a systematic review. Prenatal Diagnosis 34:205–213.
- Isaacs E, Edmonds C, Lucas A, Gadian D. 2001. Calculation difficulties in children of very low birthweight: a neural correlate. Brain 124:1701–1707.
- Jois R. 2019. Understanding long-term neurodevelopmental outcomes of very and extremely preterm infants: a clinical review. Australian Journal of General Practice 48:26–32.
- Khalil A, Rodgers M, Baschat A, Bhide A, Gratacos E, Hecher K, et al. 2016. ISUOG practice guidelines: role of ultrasound in twin pregnancy. Ultrasound in Obstetrics & Gynecology 47:247–263.
- Khalil A, Thilaganathan B. 2019. Selective fetal growth restriction in monochorionic twin pregnancy: a dilemma for clinicians and a challenge for researchers. Ultrasound in Obstetrics & Gynecology 53:23–25.
- Laganà A, Giordano D, Loddo S, Zoccali G, Vitale S, Santamaria A, et al. 2017. Decreased endothelial progenitor cells (EPCs) and increased natural killer (NK) cells in peripheral blood as possible early markers of preeclampsia: a case-control analysis. Archives of Gynecology and Obstetrics 295:867–872.
- Lewi L, Gucciardo L, Huber A, Jani J, Van Mieghem T, Doné E, et al. 2008. Clinical outcome and placental characteristics of monochorionic diamniotic twin pairs with early- and late-onset discordant growth. American Journal of Obstetrics and Gynecology 199:511.e1–511.e7.
- Mazkereth R, Miron E, Leibovitch L, Kuint J, Strauss T, Maayan-Metzger A. 2014. Growth parameters of discordant preterm twins during the first year of life. Journal of Maternal-Fetal & Neonatal Medicine 27:1795–1799.
- Morgane P, Austin-Lafrance R, Bronzino J, Tonkiss J, Díaz-Cintra S, Cintra L, et al. 1993. Prenatal malnutrition and development of the brain. Neuroscience and Biobehavioral Reviews 17:91–128.
- Morris C, Janssens A, Shilling V, Allard A, Fellowes A, Tomlinson R, et al. 2015. Meaningful health outcomes for paediatric neurodisability: stakeholder prioritisation and appropriateness of patient reported outcome measures. Health and Quality of Life Outcomes 13:87.
- Murray E, Fernandes M, Fazel M, Kennedy S, Villar J, Stein A. 2015. Differential effect of intrauterine growth restriction on childhood neurodevelopment: a systematic review. British Journal of Gynecology 122:1062–1072.
- Reolon R, Rotta N, Agranonik M, Silva A, Goldani M. 2008. Influence of intrauterine and extrauterine growth on neurodevelopmental outcome of monozygotic twins. Brazilian Journal of Medical and Biological Research 41:694–699.
- Ross G, Krauss A, Perlman J. 2012. Physical growth and cognitive abilities in concordant versus discordant birth weight twins at three years old. Early Human Development 88:753–756.
- Swamy RS, Mcconachie H, Ng J, Rankin J, Korada M, Sturgiss S, Embleton ND. 2018. Cognitive outcome in childhood of birth weight discordant monochorionic twins: the long-term effects of fetal growth restriction. Archives of Disease in Childhood. Fetal and Neonatal Edition 103:F512–F516.
- Torche F, Echevarría G. 2011. The effect of birthweight on childhood cognitive development in a middle-income country. International Journal of Epidemiology 40:1008–1018.
- Valsky D, Eixarch E, Martinez J, Crispi F, Gratacós E. 2010. Selective intrauterine growth restriction in monochorionic twins: pathophysiology, diagnostic approach and management dilemmas. Seminars in Fetal & Neonatal Medicine 15:342–348.
- Van Dommelen P, De Gunst M, Van Der Vaart A, Van Buuren S, Boomsma D. 2008. Growth references for height, weight and body mass index of twins aged 0–2.5 years. Acta Paediatrica 97:1099–1104.