

Abstract
Proteinuria during pregnancy is closely related to the occurrence of adverse pregnancy outcomes. One hundred and forty-two women with proteinuria during pregnancy and followed between January 2018 and December 2020 were evaluated. Based on the 24-h proteinuria value, they were divided as mild (n = 76, 300–1000 mg/day), moderate (n = 39, 1000–3500 mg/day) and severe (n = 27, >3500 mg/day) proteinuria. The rates of prematurity, low birth weight and neonatal asphyxia were significantly higher in the severe proteinuria group than in the mild and moderate groups, while the rates of foetal growth restriction and neonatal intensive care unit admission were significantly higher in the severe compared with the mild proteinuria group (all p < .05). Logistic regression analysis showed that moderate proteinuria (OR = 97.2, 95%CI: 7.1–1334.2, p = .001) and severe proteinuria (OR = 34.0, 95%CI: 1.6–711.0, p = .023) were associated with adverse perinatal outcomes. Compared with mild proteinuria, moderate and severe proteinuria are associated with adverse pregnancy outcomes in perinatal infants.
What is already known on this subject? The production of proteinuria is closely related to the filtration function of the glomerulus, the reabsorption and secretion function of the renal tubules. For women with normal renal function before pregnancy, such physiological changes are less likely to cause adverse symptoms; however, for women with chronic kidney disease before pregnancy, especially those with significantly impaired renal function, the kidneys often cannot compensate for these physiological changes, which can lead to serious complications for both mother and infant.
What do the results of this study add? In our study, logistic regression analysis showed that the severity of proteinuria was independently associated with adverse perinatal outcomes. The ROC curve showed that 24-h proteinuria had a predictive value for adverse perinatal outcomes. Therefore, for patients with urine protein quantification ≥0.3 g/24 h, regular 24-h urine protein quantification during pregnancy could help predict adverse perinatal outcomes and improve prognosis.
What are the implications of these findings for clinical practice and/or further research? Proteinuria quantification can be used as one of the factors predicting adverse pregnancy outcomes. Thus, monitoring of urinary protein quantification in women during pregnancy should be strengthened for early detection of renal impairment, then interventions be used to improve maternal and infant outcomes.
Impact Statement
Introduction
Significant physiological changes in women during pregnancy have significant effects on the kidneys, including hemodynamic, renal tubules functions and endocrine functions. Chronic kidney disease (CKD) affects about 3% of pregnant women (Piccoli et al. Citation2015), which is roughly equivalent to 6.4 million women each year worldwide. Women with CKD have an increased risk of adverse pregnancy outcomes, including preeclampsia, foetal growth restriction (FGR), preterm delivery and deterioration in maternal renal function (Piccoli et al. Citation2015; Barrett et al. Citation2020).
During pregnancy, because of the increase in renal blood flow and glomerular filtration rate (GFR), the glomeruli are in a state of high perfusion and high filtration. At the same time, the enlarged uterus during pregnancy compresses the renal veins, resulting in increased venous pressure and excretion of urine protein higher than in non-pregnant women. Proteinuria is a hallmark of CKD and glomerular injury and an important indicator of predicting kidney injury during pregnancy (Hutcheon et al. Citation2011). Transient proteinuria during pregnancy is mostly a physiological phenomenon, and a large amount of persistent proteinuria can lead to glomerular sclerosis, tubule-interstitial damage and end-stage renal disease (ESRD) (Zandi-Nejad et al. Citation2004), which can lead to poor pregnancy outcomes for mothers and infants. The magnitude of proteinuria can predict the outcomes of women with preeclampsia (Chan et al. Citation2005; Kumari et al. Citation2014; Lei et al. Citation2021).
Still, previous studies mainly focussed on women with preeclampsia. Therefore, this study aimed to explore the association between proteinuria and adverse pregnancy outcomes, and to detect and diagnose early, ultimately to improve maternal and infant outcomes.
Materials and methods
Study design and subjects
This retrospective cohort study included patients with proteinuria during pregnancy and followed at Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine between January 2018 and December 2020. This study was conducted retrospectively from data obtained for clinical purposes. The Bioethics Committee of Xinhua Hospital affiliated to Shanghai Jiaotong University School of Medicine was consulted and determined that this study did not need ethical approval. A Bioethics Committee’s official statement of ethical approval was granted from the Xinhua Hospital affiliated to Shanghai Jiaotong University School of Medicine. The study was conducted according to the principles of the Declaration of Helsinki and its amendments. There was no requirement for individual informed consent.
The inclusion criteria were (1) diagnosed with proteinuria during pregnancy according to laboratory examination results and (2) urine protein quantification on different days >0.3 g/24 h. The exclusion criteria were (1) those without periodic prenatal check-up data, (2) those without birth records or newborn records or (3) those with incomplete laboratory or auxiliary examination data.
Data collection and definitions
The demographic and clinical characteristics of the patients were collected, including age, gestational week, gravidity, parity, body mass index (BMI), blood pressure at the first prenatal check-up, blood pressure during hospitalisation, history of kidney disease, blood urea nitrogen (BUN), serum creatinine (SCr), serum uric acid (UA), estimated GFR (eGFR), aspartate transaminase (AST), alanine transaminase (ALT), platelet count, serum albumin, 24-h proteinuria value, renal insufficiency, anaemia, hypoproteinemia, preeclampsia and adverse pregnancy outcomes.
The patients were divided into three groups according to the degrees of proteinuria: mild proteinuria (300 mg≤ 24-h proteinuria<1000 mg), moderate proteinuria (1000≤ 24-h proteinuria ≤3500 mg) and severe proteinuria (24-h proteinuria of >3500 mg) (Thornton et al. Citation2010; Anon Citation2019). In this study, the 24-h proteinuria value was the average value of the multiple test results on different days after discovering proteinuria.
Renal insufficiency was defined as SCr ≥71 µmol/L during pregnancy (Gurrieri et al. Citation2012). Gestational age at the time of proteinuria was classified as early pregnancy (<12 weeks), second trimester (12–28 weeks) and late pregnancy (>28 weeks). Anaemia during pregnancy was defined as haemoglobin (Hb) <110 g/L (Black et al. Citation2013). Hypoproteinemia during pregnancy was defined as serum albumin <30 g/L (Chen et al. Citation2016). Preeclampsia was diagnosed according to the guidelines for the diagnosis and treatment of hypertensive disorder in pregnancy (2015 Edition) (Pregnancy Hypertension Group of Obstetrics and Gynecology Branch of Chinese Medical Association Citation2016).
Adverse maternal outcomes included caesarean section, severe preeclampsia, placenta abruption, anaemia during pregnancy, hypoproteinemia, renal insufficiency, haemolysis, elevated liver enzymes and low platelet count (HELLP) syndrome and maternal death. The adverse perinatal outcomes were premature birth (<37 weeks), neonatal asphyxia (Apgar score ≤7 points at 1 min after birth; Zou et al. Citation2017), foetal distress, FGR, low birth weight (LBW)/very low birth weight (VLBW), neonatal admission to the intensive care unit (NICU) or perinatal death.
Statistical analysis
The statistical analyses were performed using SPSS 23.0 (IBM Corp., Armonk, NY). The Shapiro–Wilk test was used to test the normality of the continuous variables. The continuous variables with a normal distribution were presented using means ± standard deviation (SD) and compared among groups using ANOVA and Student’s t-test. Continuous with a skewed distribution were presented using medians and interquartile range and analysed using the Kruskal–Wallis H test. Categorical variables were presented using frequency and percentage (%) and compared among the groups using the chi-square test. A logistic regression analysis of proteinuria severity for adverse pregnancy outcomes was performed. The receiver operating characteristic (ROC) curve was used to evaluate the ability of the 24-h proteinuria value to distinguish the adverse pregnancy outcomes. p Values <.05 were considered statistically significant.
Results
Characteristics of the patients
A total of 142 pregnant women with proteinuria were included. They were 32.0 ± 4.8 years old. The gestational age at delivery was 36.1 ± 3.5 weeks. The 24-h proteinuria value was 1911 (450, 2560) mg/day. Among the 142 women, 21 (14.8%) had renal insufficiency during pregnancy, 104 (73.2%) had hypertension, 16 (11.3%) had anaemia, 39 (27.5%) had hypoproteinemia and four (2.8%) had acute kidney injury (AKI).
There were 76, 34 and 27 women in the mild, moderate and severe proteinuria groups. The systolic blood pressure (SBP), diastolic blood pressure (DBP), BUN and serum UA levels in the moderate and severe proteinuria group were significantly higher than in the mild proteinuria group (all p < .05). The gestational age at childbirth was lower than in the mild proteinuria group (p < .05) ().
Table 1. Clinical characteristics of the patients.
Comparison of maternal outcomes
The frequency of hypoalbuminemia in the moderate proteinuria group was higher than in the mild proteinuria group (p < .01). The frequency of HELLP syndrome in the severe proteinuria group was higher than in the mild proteinuria group (p < .05), and the frequencies of severe PE, anaemia and hypoproteinemia were higher than in the mild proteinuria group (p < .01). The frequencies of severe PE and hypoalbuminemia in the severe proteinuria group were higher than in the moderate proteinuria group (p < .01) ().
Table 2. Comparison of pregnancy outcomes.
Comparison of perinatal outcomes
The frequencies of prematurity and FGR in the moderate proteinuria group were higher than in the mild proteinuria group (p < .05). The LBW/VLBW and NICU frequencies were higher than in the mild proteinuria group (p < .01). The head circumference and Apgar at 1 min were lower than in the mild proteinuria group (p < .05), and the weight and length of the newborns were lower than in the mild proteinuria group (p < .01). There were no significant differences in foetal intrauterine distress or perinatal death rates between the severe and mild groups, while all other adverse outcomes were more common in the severe group compared with the mild group (p < .01). The frequency of prematurity in the severe group was higher than in the moderate proteinuria group (p < .05). The neonatal asphyxia and LBW/VLBW rates were higher than in the moderate proteinuria group (p < .01), while the weight and length of the newborns and the Apgar 1-minute score were lower than in the moderate proteinuria group (p < .01) ().
Table 3. Comparison of perinatal outcomes.
Analysis of pregnancy outcomes and risk factors
As the patients with good maternal outcomes were all in the mild proteinuria group and the patients with poor maternal outcomes were all in the moderate or severe proteinuria group, multivariable analysis of the maternal outcomes could not be performed.
Among the 142 births, 74 (52.1%) had poor perinatal outcomes, including two perinatal deaths, nine with foetal distress, 17 with neonatal asphyxia, three with placental abruption, 51 with prematurity and 58 with NICU admission (multiple poor outcomes could be observed in a single child). Logistic regression analysis showed that moderate proteinuria (OR = 59.2, 95%CI: 1.29–2715.80, p = .044) and severe proteinuria (OR = 72.3, 95%CI: 1.29–4015.56, p = .041) were independently associated with adverse perinatal outcomes (Table S1).
24-h Proteinuria cut-off value to predict adverse perinatal outcomes
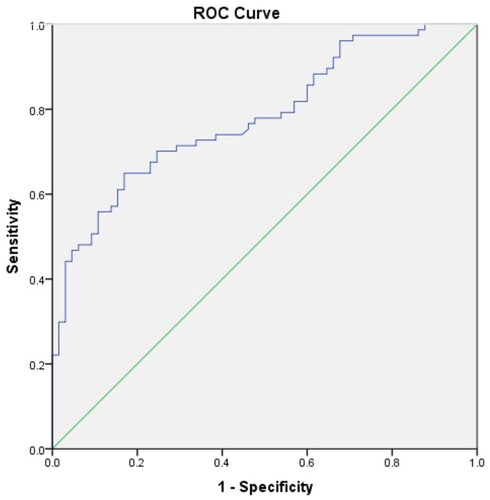
The ROC curve analysis results of adverse perinatal outcomes showed that the area under the curve was 0.782, and the critical value (according to the Youden index) was the maximum proteinuria of 1125.5 mg/24 h, resulting in 65% sensitivity and 17% specificity (p < .001) ().
Figure 1. 24-h proteinuria cut-off value to predict adverse perinatal outcomes.
Discussion
This study explored the association between proteinuria and adverse pregnancy outcomes in pregnant women. The results showed that moderate and severe proteinuria is associated with adverse pregnancy outcomes in patients with proteinuria during pregnancy. Hence, urine protein quantification could be used as a predictive evaluation index for maternal and perinatal outcomes.
Proteinuria during pregnancy is related to the glomerular filtration and the reabsorption and secretion of renal tubules (Cheung and Lafayette Citation2013; Conrad and Davison Citation2014). Under normal pregnancy conditions, due to the charge barrier and the pore barrier, the large and medium molecular weight proteins in the plasma cannot pass through the glomerulus, whereas the small molecular proteins can pass (Cheung and Lafayette Citation2013; Conrad and Davison Citation2014). The proximal convoluted tubule reabsorbs more than 95% of the proteins, and the final protein content in the final urine is 30–130 mg/24 h. In the third trimester of pregnancy, women’s GFR can increase by 40–50%, and protein filtration increases accordingly, reaching 0.25–0.30 g/24 h (Hladunewich Citation2017). For women with normal renal function before pregnancy, this physiological proteinuria will not cause adverse pregnancy outcomes, but for women with a history of CKD, it will often cause adverse maternal and perinatal outcomes (Krane and Hamrahian Citation2007). A 24-h proteinuria >0.3 g is considered renal injury (Maynard and Thadhani Citation2009) and >2 g is substantial proteinuria (Li et al. Citation2018). If proteinuria continues to be positive for more than 12 weeks after the end of pregnancy, it may indicate CKD. Persistent proteinuria can cause renal injury and promote the development of CKD (Schmieder et al. Citation2011; Usui et al. Citation2018). Jungers et al. (Citation1995) and Prakash (Citation2012) have shown that pregnant women with proteinuria >1 g/24 h are more likely to have a decline in GFR after the end of pregnancy, and proteinuria will still have a persistent adverse effect on women’s renal function (Shahbazian et al. Citation2011), and the risk of a progression to ESRD is likely. High proteinuria puts pregnant women at risk of hypoalbuminemia, organ dysfunction, retinal arteriole spasm and retinal detachment (Lei et al. Citation2021), which has varying degrees of impact on maternal and perinatal outcomes.
Proteinuria during pregnancy is a common disease in obstetrics. It can be caused by complications during pregnancy, such as hypertension, HELLP syndrome, chronic glomerulonephritis, nephrotic syndrome and immune diseases (Cheung and Lafayette Citation2013; Conrad and Davison Citation2014). Hypertension in pregnancy can cause systemic arteriole spasms, reduced placental blood flow and restricted foetal growth, leading to foetal distress and adverse pregnancy outcomes (Xu et al. Citation2020). In patients with PE, renal vasospasm, damage to the glomerular basement membrane, and increased permeability of the glomerular filtration membrane may be one of the reasons for the occurrence of proteinuria. The pathological basis of PE is arteriolar spasm, which can involve multiple organs (Tomimatsu et al. Citation2019), and the kidney is one of the main organs involved, and severe cases can manifest as acute renal failure. The placenta plays an important role in the pathogenesis and progression of preeclampsia. Two-stage model gradually became widely accepted by scholars. The first stage is in early pregnancy, due to the lack of high-flow and low-resistance spiral arteries, the placental perfusion is reduced and placental development is blocked, various placental developmental defects lead to insufficient blood supply at the maternal–foetal interface (Staff Citation2019); the second stage is in second trimester, when placental function fails to meet the normal pregnancy so as lead to a state of ischaemia and hypoxia of the uterus-placenta for a long time. The HELLP syndrome is a serious complication of hypertension in pregnancy, and its pathogenesis is similar to preeclampsia, including abnormal placental function, activation of the immune system, and endothelial dysfunction (Wallace et al. Citation2018). In this study, 104 (73.2%) of the pregnant women had hypertension during pregnancy, 54 (38.0%) developed severe preeclampsia, and nine (6.3%) had HELLP syndrome. The overall frequency of adverse maternal outcomes in the 142 patients with proteinuria during pregnancy reached 77.5%, similar to literature reports.
The occurrence of adverse pregnancy outcomes was higher in the severe proteinuria group compared with the mild group. An increase in proteinuria is directly related to adverse maternal and perinatal outcomes (Yılmaz Baran et al. Citation2020). Bramham et al. (Citation2013) showed that the pregnancy outcomes of pregnant women with proteinuria >0.5 g/24 h were worse than in women with 0.3 g/24 h, including premature delivery, severe hypertension, and the need for magnesium sulphate treatment during pregnancy, indicating that proteinuria can be used as a predictor of adverse pregnancy outcomes. Piccoli et al. (Citation2010) found that the risk of premature delivery and neonatal admission to NICU in women with proteinuria >1 g/24 h was higher than that for normal pregnancy. Wiles et al. (Citation2019) believe that even asymptomatic proteinuria in the first trimester (>0.5 g/24 h) will increase the incidence of preterm delivery and FGR.
In this study, we divided the patients into three groups with different degrees of urine protein quantification. We found that the incidence of PE and hypoproteinemia in the severe proteinuria group was higher than that in the moderate group, and the incidence of hypoproteinemia in the moderate group was higher than that in the mild proteinuria group. Both hypoproteinemia and PE were regarded as one of the adverse outcomes of mothers, thus indicating that with the increase in the degree of proteinuria during pregnancy, the proportion of maternal adverse outcomes increased. Similarly, we found that the severe proteinuria group had higher neonatal adverse outcomes, including preterm birth rate, neonatal asphyxia rate, and incidence of LBW/VLBW than those in the moderate group, while birth weight and 1-min Apgar score were significantly lower than those in the moderate group. Hence, the occurrence of adverse perinatal outcomes of the patients in the severe proteinuria group was significantly higher than that in the mild and moderate proteinuria group. Logistic regression analysis showed that the severity of proteinuria was independently associated with adverse perinatal outcomes. The ROC curve showed that 24-h proteinuria had a predictive value for adverse perinatal outcomes. Therefore, for patients with urine protein quantification ≥0.3 g/24 h, regular 24-h urine protein quantification during pregnancy could help predict adverse perinatal outcomes and improve prognosis.
This study has limitations. It was performed at a single hospital, and the sample size was small. It was a retrospective study, and the data were limited to those available in the charts. Only patients with proteinuria were included, and there was no group of women with normal urinary protein levels. The adverse maternal outcomes could not be analysed using multivariable analyses because all women with good outcomes were in the mild group. As the sample size of moderate proteinuria and severe proteinuria was small, the OR and 95%CI were large. Additional studies with larger sample size are necessary to determine the exact predictive values of urinary protein for adverse pregnancy outcomes.
In conclusion, moderate and severe proteinuria are independently associated with adverse pregnancy outcomes in patients with proteinuria during pregnancy. Proteinuria quantification can be used as one of the factors predicting adverse pregnancy outcomes.
Author contributions
HMJ and LW carried out the retrospective review of the data and participated in the design, writing and organisation of the manuscript. LW conceived the study and designed it. HMJ participated in the collection and analysis of data. The final version of the manuscript has been read and approved by all authors.
Supplemental Material
Download MS Word (14.9 KB)Acknowledgements
We would like to acknowledge the whole team members involved in the management.
Disclosure statement
The authors report no conflict of interest.
Data availability statement
The datasets used and analysed during the current study are available from the corresponding author on reasonable request.
Additional information
Funding
References
- Anon. 2019. ACOG Practice Bulletin No. 202: gestational hypertension and preeclampsia. Obstetrics & Gynecology 133:1.
- Barrett PM, McCarthy FP, Kublickiene K, Cormican S, Judge C, Evans M, et al. 2020. Adverse pregnancy outcomes and long-term maternal kidney disease: a systematic review and meta-analysis. JAMA Network Open 3:e1920964.
- Black RE, Victora CG, Walker SP, Bhutta ZA, Christian P, De Onis M, et al. 2013. Maternal and child undernutrition and overweight in low-income and middle-income countries. Lancet 382:427–451.
- Bramham K, Poli-De-Figueiredo CE, Seed PT, Briley AL, Poston L, Shennan AH, Chappell LC. 2013. Association of proteinuria threshold in pre-eclampsia with maternal and perinatal outcomes: a nested case control cohort of high risk women. PLOS One 8:e76083.
- Chan P, Brown M, Simpson JM, Davis G. 2005. Proteinuria in pre-eclampsia: how much matters? British Journal of Gynecology 112:280–285.
- Chen H, Tao F, Fang X, Wang X. 2016. Association of hypoproteinemia in preeclampsia with maternal and perinatal outcomes: a retrospective analysis of high-risk women. Journal of Research in Medical Sciences 21:98.
- Cheung KL, Lafayette RA. 2013. Renal physiology of pregnancy. Advances in Chronic Kidney Disease 20:209–214.
- Conrad KP, Davison JM. 2014. The renal circulation in normal pregnancy and preeclampsia: is there a place for relaxin? American Journal of Physiology. Renal Physiology 306:F1121–F1135.
- Gurrieri C, Garovic VD, Gullo A, Bojanic K, Sprung J, Narr BJ, Weingarten TN. 2012. Kidney injury during pregnancy: associated comorbid conditions and outcomes. Archives of Gynecology and Obstetrics 286:567–573.
- Hladunewich MA. 2017. Chronic kidney disease and pregnancy. Seminars in Nephrology 37:337–346.
- Hutcheon JA, Lisonkova S, Joseph KS. 2011. Epidemiology of pre-eclampsia and the other hypertensive disorders of pregnancy. Best Practice & Research. Clinical Obstetrics & Gynaecology 25:391–403.
- Jungers P, Houillier P, Forget D, Labrunie M, Skhiri H, Giatras I, Descamps-Latscha B. 1995. Influence of pregnancy on the course of primary chronic glomerulonephritis. Lancet 346:1122–1124.
- Krane NK, Hamrahian M. 2007. Pregnancy: kidney diseases and hypertension. American Journal of Kidney Diseases 49:336–345.
- Kumari A, Chakrawarty A, Singh A, Singh R. 2014. Maternofoetal complications and their association with proteinuria in a tertiary care hospital of a developing country. Journal of Pregnancy 2014:431837.
- Lei T, Qiu T, Liao W, Li K, Lai X, Huang H, et al. 2021. Proteinuria may be an indicator of adverse pregnancy outcomes in patients with preeclampsia: a retrospective study. Reproductive Biology and Endocrinology 19:71.
- Li B, Lin L, Yang H, Zhu Y, Wei Y, Li X, et al. 2018. The value of the 24-h proteinuria in evaluating the severity of preeclampsia and predicting its adverse maternal outcomes. Hypertension in Pregnancy 37:118–125.
- Maynard SE, Thadhani R. 2009. Pregnancy and the kidney. Journal of the American Society of Nephrology 20:14–22.
- Piccoli GB, Attini R, Vasario E, Conijn A, Biolcati M, D'amico F, et al. 2010. Pregnancy and chronic kidney disease: a challenge in all CKD stages. Clinical Journal of the American Society of Nephrology 5:844–855.
- Piccoli GB, Cabiddu G, Attini R, Vigotti FN, Maxia S, Lepori N, et al. 2015. Risk of adverse pregnancy outcomes in women with CKD. Journal of the American Society of Nephrology 26:2011–2022.
- Prakash J. 2012. The kidney in pregnancy: a journey of three decades. Indian Journal of Nephrology 22:159–167.
- Pregnancy Hypertension Group of Obstetrics and Gynecology Branch of Chinese Medical Association. 2016. Guidelines for the diagnosis and treatment of hypertensive disorders complicating pregnancy (2015). Chinese Journal of Obstetrics and Gynecology 19:161–169.
- Schmieder RE, Mann JF, Schumacher H, Gao P, Mancia G, Weber MA, et al. 2011. Changes in albuminuria predict mortality and morbidity in patients with vascular disease. Journal of the American Society of Nephrology 22:1353–1364.
- Shahbazian N, Shahbazian H, Ehsanpour A, Aref A, Gharibzadeh S. 2011. Hypertension and microalbuminuria 5 years after pregnancies complicated by pre-eclampsia. Iranian Journal of Kidney Diseases 5:324–327.
- Staff AC. 2019. The two-stage placental model of preeclampsia: an update. Journal of Reproductive Immunology 134–135:1–10.
- Thornton CE, Makris A, Ogle RF, Tooher JM, Hennessy A. 2010. Role of proteinuria in defining pre-eclampsia: clinical outcomes for women and babies. Clinical and Experimental Pharmacology and Physiology 37:466–470.
- Tomimatsu T, Mimura K, Matsuzaki S, Endo M, Kumasawa K, Kimura T. 2019. Preeclampsia: maternal systemic vascular disorder caused by generalized endothelial dysfunction due to placental antiangiogenic factors. International Journal of Molecular Sciences 20:42–46.
- Usui T, Kanda E, Iseki C, Iseki K, Kashihara N, Nangaku M. 2018. Observation period for changes in proteinuria and risk prediction of end-stage renal disease in general population. Nephrology 23:821–829.
- Wallace K, Harris S, Addison A, Bean C. 2018. HELLP syndrome: pathophysiology and current therapies. Current Pharmaceutical Biotechnology 19:816–826.
- Wiles K, Chappell L, Clark K, Elman L, Hall M, Lightstone L, et al. 2019. Clinical practice guideline on pregnancy and renal disease. BMC Nephrology 20:401.
- Xu X, Wang Y, Xu H, Kang Y, Zhu Q. 2020. Association between proteinuria and maternal and neonatal outcomes in pre-eclampsia pregnancy: a retrospective observational study. Journal of International Medical Research 48:300060520908114.
- Yılmaz Baran Ş, Alemdaroğlu S, Durdağ GD, Yetkinel S, Yüksel Şimşek S, Kalaycı H, Şimşek E. 2020. Reappraisal of the relationship between 24-hour proteinuria and preeclampsia in terms of the maternal and perinatal outcomes. Hypertension in Pregnancy 39:82–88.
- Zandi-Nejad K, Eddy AA, Glassock RJ, Brenner BM. 2004. Why is proteinuria an ominous biomarker of progressive kidney disease? Kidney International 66:S76–S89.
- Zou YS, Guo Y, Cheng R, Zhou XG, Cao ZL. 2017. Diagnostic values of prealbumin and retinol-binding protein for liver damage caused by different degrees of neonatal asphyxia. Zhongguo Dang Dai Er Ke Za Zhi 19:337–341.