

Introduction
Mesothelioma is a primary tumour originating mostly from mesothelial cells lining the pleura, and more rarely from peritoneum and pericardium (Sterman et al. Citation1999). Peritoneal malignant mesotheliomas are aggressive tumours (Alexander and Burke Citation2016). They constitute 15–33% of all malignant mesothelioma cases (Ohya et al. Citation2019). Patients with peritoneal malignant mesothelioma present with peritoneal thickening and irregularity, peritoneal masses, diffuse ascites, lymph node enlargement and/or adnexal masses, and imaging reveals mesenteric tissue irregularity and metastasis to distant or adjacent organs. The most common clinical findings are ascites, nausea, vomiting, abdominal pain, weight loss, fever, diarrhoea, anorexia, early satiety and fatigue (Liang et al. Citation2016).
In this article, we aimed to present two cases of primary peritoneal malignant mesothelioma mimicking peritonitis carcinomatosis, clinically. Although the initial diagnosis in patients with similar clinical findings is advanced stage ovarian cancer, mesothelioma may be considered in the differential diagnosis in patients who have undergone hysterectomy and bilateral salpingo-oophorectomy. Our study does not have any ethics committee approval due to the nature of the study design.
Case presentation
Case 1
A female patient, aged 76, admitted to emergency room owing to shortness of breath and abdominal distension for 1 month. On transvaginal ultrasonography (TvUSG), 9 cm of free fluid was noted in the pouch of Douglas without any pelvic mass. Two thousand millilitres of fluid was removed during paracentesis. She had a history of hysterectomy and bilateral salpingo-oophorectomy (TAH + BSO) due to uterine fibroid 30 years earlier. On pelvic magnetic resonance imaging (MRI), there was thickening and contrast enhancement on the peritoneal planes which were more prominent in both paracolic areas. Mass lesions were detected as diffusion limiting soft tissue densities consistent with peritonitis carcinomatosis. Nodular lesions, the largest 15 × 11 mm in size, were observed in the posterolateral aspect of the liver capsule which was indicating the protrusion of a metastatic implant into the parenchyma.
On positron emission tomography (PET)-CT, linear abnormal uptake was observed in the peritoneal surfaces. The thickest part of the omental cake had a maximum standardized uptake (SUVmax) value of 12. Diagnostic laparoscopy was performed following patient’s contest.
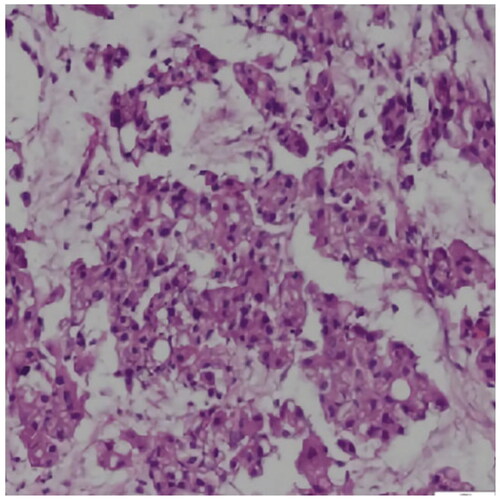
Multiple miliary nodular implants involving all peritoneal surfaces were noted intraoperatively. Biopsies were obtained from the peritoneal surfaces and omentum. The final pathological diagnosis was malignant epithelioid mesothelioma () involving omentum. Staining with periodic acid-Schiff (PAS) and PAS with diastase (PAS-D) were positive. Immunohistochemical staining for CA125, D2-40, cytokeratin (CK) 5/6 and calretinin was positive, and wild-type staining was observed with p53.
Figure 1. Photomicrograph of malignant epithelioid mesothelioma showing relatively large malignant cells with abundant eosinophilic cytoplasm and round to oval nuclei (H and E ×40) (case 1).
The patient was administered one cycle of chemotherapy, but she died due to respiratory arrest 5 months after the diagnosis.
Case 2
A female patient, aged 59, had undergone TAH + BSO 10 years earlier. She was admitted to hospital with complaint of shortness of breath in October 2020. On CT, ascites, bilateral pleural effusion and a lesion measuring 90 mm×60 mm that was compatible with peritonitis carcinomatosis in the pelvis, omentum and mesentery were detected. Pathological analysis of omental biopsy indicated serous carcinoma, and the patient received chemotherapy. She was then referred to our clinic for debulking surgery. No pelvic masses or ascites were observed on TvUSG.
Heterogeneous densities near the liver, small lesions, especially in the mesentery in the anterior abdominopelvic junction, and findings consistent with lymphadenopathy (LAP) in the retroperitoneum were also noted on CT. PET-CT revealed lesions with diffuse hypermetabolic (SUVmax: 7.3) density involving almost the entire pelvis. The pathological diagnosis was malignant epithelioid mesothelioma after re-evaluation of the patient’s pre-existing tissue preparations. Staining for D2-40, calretinin and WT-1 was positive, and focal positive staining for CK5/6 was observed in the immunohistochemical stains.
Medical treatment could not be administered to the patient since she was out of follow-up.
Discussion
Peritoneal carcinomatosis is defined as intraperitoneal spread of any tumour that does not originate in the peritoneum itself. To avoid unnecessary surgical interventions, a careful differential diagnosis should be made.
Mesothelioma is a rare and aggressive primary tumour originating from the pleural, pericardial and peritoneal membranes. Peritoneal involvement has been reported in 25% of affected patients (Smiti and Rajagopal Citation2010). Studies have reported that diffuse malignant mesothelioma of the peritoneum developed owing to chronic inflammation (Butnor et al. Citation2017) but both patients had no history of such disease.
The macroscopic features of mesothelioma are similar to those of peritoneal carcinomatosis, namely ascites, diffuse and/or nodular thickening of the peritoneal membranes, omental cake and mesenteric masses. The typical CT findings of peritoneal carcinomatosis are multifocal discrete nodules, infiltrative masses in the peritoneal cavity, omental opacity, ascites and peritoneal thickening (Li and Alexander Citation2018). Both of our patients had findings consistent with mesothelioma, which should be considered in the differential diagnosis of peritoneal carcinomatosis.
Malignant mesothelioma can be challenging to diagnose (Boussios et al. Citation2018). Histopathological examination is essential for accurate diagnosis. CT, MRI and PET are the main imaging modalities without pathognomonic findings (Boussios et al. Citation2018). Abdominal cytology is generally of low diagnostic value (Kim et al. Citation2017).
Conclusions
In cases of peritoneal carcinomatosis, mesothelioma is among the differential diagnoses that should be considered because these conditions are both associated with many common clinical and radiological features.
Disclosure statement
No potential conflict of interest was reported by the author(s).
References
- Alexander, H.R. Jr. and Burke, A.P., 2016. Diagnosis and management of patients with malignant peritoneal mesothelioma. Journal of Gastrointestinal Oncology, 7 (1), 79–86.
- Boussios, S., et al., 2018. Malignant peritoneal mesothelioma: clinical aspects, and therapeutic perspectives. Annals of Gastroenterology, 31 (6), 659–669.
- Butnor, K.J., et al., 2017. Malignant peritoneal mesothelioma and Crohn disease. Journal of Clinical Pathology, 70 (3), 228–232.
- Kim, J., Bhagwandin, S., and Labow, D.M., 2017. Malignant peritoneal mesothelioma: a review. Annals of Translational Medicine, 5 (11), 236.
- Li, C.Y. and Alexander, H.R. Jr., 2018. Peritoneal metastases from malignant mesothelioma. Surgical Oncology Clinics of North America, 27 (3), 539–549.
- Liang, Y.F., et al., 2016. CT differentiation of diffuse malignant peritoneal mesothelioma and peritoneal carcinomatosis. Journal of Gastroenterology and Hepatology, 31 (4), 709–715.
- Ohya, M., et al., 2019. Malignant peritoneal mesothelioma diagnosed 50 years postradiotherapy for ovarian cancer in a patient with a history of multiple malignancies: an autopsy case. Molecular and Clinical Oncology, 11 (4), 397–400.
- Smiti, S. and Rajagopal, K., 2010. CT mimics of peritoneal carcinomatosis. Indian Journal of Radiology & İmaging, 20 (1), 58–62.
- Sterman, D.H., Kaiser, L.R., and Albelda, S.M., 1999. Advances in the treatment of malignant pleural mesothelioma. Chest, 116 (2), 504–520.