

Abstract
Scrub typhus, caused by Orientia tsutsugamushi, is a re-emerging endemic zoonosis in the Asia Pacific region. It is a febrile condition ranging in severity from mild to severe, with fatality rates as high as 30%. The present study aims towards analysing the clinical profile and pregnancy outcomes in 27 cases of scrub typhus admitted to a tertiary care centre in North India. The medical records of 27 pregnant women who had scrub typhus were analysed. The IgM ELISA was used to look for IgM antibodies to Orientia tsutsugamushi in the patient’s serum sample. An optical density of more than or equal to 0.468 was considered as positive. Majority of the pregnant females delivered healthy and live babies. However, poor foetal outcomes were observed in four (14.8%) cases with intrauterine deaths occurring in two (7.4%) cases and still birth in one (3.7%) case, while one (3.7%) patient had spontaneous abortion. Maternal mortality was reported in one patient (3.7%) due to a delay in diagnosis. In endemic settings, a strong index of suspicion for scrub typhus is necessary in pregnant females presenting with fever. The key to reducing morbidity in both the mother and foetus is early diagnosis and treatment.
What is already known on this subject? Scrub typhus is a febrile condition ranging in severity from mild to severe, with 30% mortality in untreated patients.
What do the results of this study add? Majority of the pregnant females delivered healthy and live babies. However, poor foetal outcomes were observed in four (14.8%) cases with intrauterine deaths occurring in two (7.4%) cases and still birth in one (3.7%) case, while one (3.7%) patient had spontaneous abortion. Maternal mortality was reported in one patient (3.7%) due to a delay in diagnosis.
What are the implications of these findings for clinical practice and/or further research? In endemic settings, a strong index of suspicion for scrub typhus is necessary for pregnant females presenting with fever. The key to reducing morbidity in both the mother and foetus is early diagnosis and treatment.
Impact Statement
Introduction
Scrub typhus, caused by mite-borne intracellular bacterium Orientia tsutsugamushi, is widely prevalent endemic zoonosis in the region of Asia-Pacific, affecting almost a million people every year (Jensenius et al. Citation2004, Tseng et al. Citation2008). Scrub typhus is re-emerging in India with several outbreaks reported in the last decade (Lakshmi et al. Citation2020). Infections can be acquired in rural, semi-urban and urban regions and thus it threatens one billion human populations globally (McCrumb et al. Citation1957, Jensenius et al. Citation2004, Elliott et al. Citation2019).
The clinical manifestations of scrub typhus include flu-like symptoms, fever, maculopapular rash, eschar, headache, cough, myalgia, lymphadenopathy, vomiting and abdominal pain (Xu et al. Citation2017). In a few cases, the disease progresses to multi-organ failure and death (Peter et al. Citation2015). The case fatality rate (CFR) is 30% or even higher in untreated cases (Rajan et al. Citation2016). It is a major cause of acute undifferentiated febrile illness (AUFI) in India, with high CFR and a link to adverse foetal outcomes in pregnant women having the illness (Kim et al. Citation2006, Chrispal et al. Citation2010). Despite the fact that scrub typhus is uncommon during pregnancy and the influence of scrub typhus on pregnancy is unknown, few research suggests that it is linked to adverse pregnancy outcomes (Watt et al. Citation1999, Mathai et al. Citation2003, Phupong and Srettakraikul Citation2004). Therefore, the aim of the present study was to evaluate the clinical outcome of scrub typhus infection in pregnancy.
Materials and methods
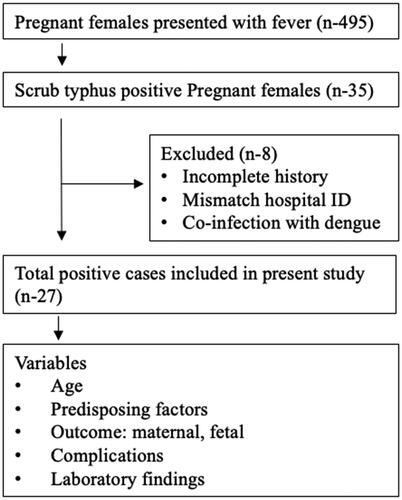
The present study was a retrospective. The case records of pregnant females diagnosed with scrub typhus at the Postgraduate Institute of Medical Education and Research, Chandigarh, India, between January 2016 and March 2021 were reviewed. Over this period, 495 pregnant females with fever were admitted to the Obstetrics and Gynaecology ward of our hospital. Febrile workup was carried out in all the cases and found negative for malaria, typhoid, leptospirosis and dengue. In addition, urine cultures and blood cultures did not show any significant growth.
Based on WHO criteria (World Health Organization Citation2012), a total of 35 pregnant females were diagnosed with scrub typhus. However, eight patients were excluded due to inadequate history, mismatched hospital ID and co-infection with dengue. A total 27 pregnant females, were recruited to the study; to diagnose scrub typhus. The serology was done by IgM ELISA kit (InBios International Inc., Seattle, WA) to detect IgM antibodies to Orientia tsutsugamushi in the patient’s serum. The test was carried out according to manufacturer’s instructions, with an optical density (OD) of more than or equal to 0.468 indicating a positive result. The details of data collection methodology are described in .
Figure 1. The data collection methodology.
Results
All 27 pregnant patients included in the study were younger than 40 years (range, 19–40 years; mean 27.85 ± 4.6 years). One (3.7%) patient presented in the first trimester when she developed the disease; two (7.4%) and 20 patients (74.1%) presented in their second and third trimester, respectively. The remaining four (14.8%) patients presented in their postpartum period.
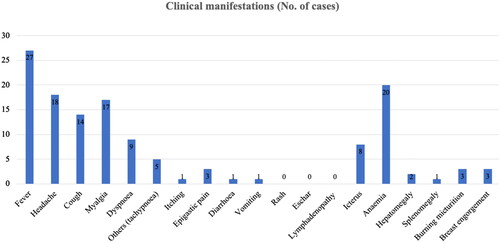
The predominant symptoms were fever (n = 27, 100%), headache (n = 18, 66.7%), myalgia (n = 17, 62.9%), cough (n = 14, 51.9%) and dyspnoea (n = 9, 33.3%). The majority of them had high grade intermittent fever of <7 days duration. Icterus (n = 8, 29.6%) and anaemia (n = 20, 74%) were the predominant clinical signs. One patient who had jaundice was HEV positive and developed hepatic encephalopathy in the later course of the disease. None of the patients had maculopapular rash, lymphadenopathy or an eschar. The clinical manifestations are shown in .
Figure 2. Clinical spectrum of pregnant patients with scrub typhus.
Laboratory findings: Most of the patients had raised liver enzymes such as: aspartate aminotransferase (88.9%), alanine aminotransferase (70.4%) and alkaline phosphatase (85.2%) in the serum. Hyperbilirubinaemia was seen in 13 (48.1%) patients and eight (29.6%) of them had thrombocytopenia. Leucocytosis was seen in 10 (37%) patients. Laboratory findings are summarised in .
Table 1. Biochemical parameters of pregnant patient with scrub typhus in a tertiary care hospital.
The associated medical risk factors such as: seizure disorder (n = 2), tuberculosis (n = 2), hypothyroidism (n = 1), valvular heart disease (n = 3), and Rh incompatibility (n = 1) were present in nine patients. Of the three patients with valvular heart disease, one patient had a spontaneous abortion. One (3.7%) patient had history of recurrent pregnancy loss.
In general complications, AKI was found in two (7.4%) cases, acute respiratory distress syndrome (ARDS) occurred in one (3.7%) case. One patient (3.7%) developed pleural effusion and four (14.8%) cases exhibit multiple organ dysfunction syndrome (MODS). In obstetric complications: oligohydramnios, anhydramnios and antepartum haemorrhage (APH) occurred in two (7.40%), one (3.70%) and two (7.40%) cases, respectively, as depicted in .
Figure 3. Complications in pregnant females with scrub typhus.
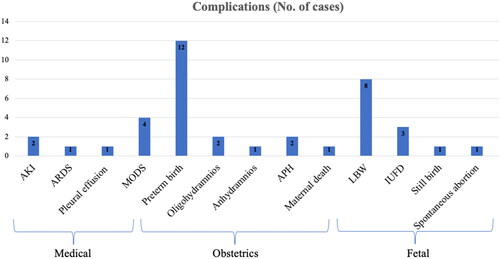
Vaginal delivery was the dominant mode of delivery observed in 16 (59.3%) cases, while caesarean delivery was done in nine (33.3%) obstetric cases. The gestational age at the time of admission was variable, ranging from 10 to 38 weeks. Preterm delivery was done in 12 (44.4%) patients. Majority of them delivered healthy and live babies weighing from 1100 to 3500 g. Among the total 19 live births, eight (42.1%) newborns had low birth weight. Poor foetal outcomes were observed in five (18.5%) pregnancies with three (11.1%) intrauterine deaths and one (3.7%) still birth, while one (3.7%) patient had spontaneous abortion at 10 weeks of gestation. Maternal mortality was reported in one patient (3.7%) due to delayed diagnosis followed by delay in initiation of appropriate treatment. Patients who visited in their ante-natal period were managed with azithromycin, while doxycycline was used for the patients after abortion or post-delivery as treatment.
IgM ELISA is a reliable test for serological confirmation of scrub typhus. The OD value of IgM scrub ELISA in the present study was between 0.493 and 4, with a mean of 1.47 OD value ranges from 0.487 to 0.500; 0.500–1.00 and >1 in one (3.7%), nine (33.3%) and 17 (63%) patients, respectively. In our experience, OD value of greater than or equal to 1.0 has a high specificity for scrub typhus in pregnant females.
Discussion
Tropical infections, such as leptospirosis, enteric fever, malaria, dengue and scrub typhus are the prevalent cause of AUFI (Chrispal et al. Citation2010, Gaba et al. Citation2020). In North India, scrub typhus is a prevalent cause of non-specific febrile illness (Mahajan Citation2005, Bhat et al. Citation2014, Oberoi and Varghese Citation2014). Scrub typhus morbidity and mortality are expected to rise in low- and middle-income nations due to inadequate reproductive health care in rural regions. In semi-arid locations, urbanisation mixed with deforestation exposes a growing number of people to these vectors, and primary care physicians, on the other hand, have just a rudimentary understanding of the condition.
The clinical features in the present study are in concordance with other studies with fever, headache, cough and myalgia being the predominant symptoms (Sivarajan et al. Citation2016). It is a tedious task to discriminate scrub typhus from other co-existing tropical illnesses based on the non-specific presentation. Therefore, a high index of clinical suspicion along with detailed history of environmental exposure, and careful examination for the eschar are critical for diagnosis (Sivarajan et al. Citation2016). However, in the present study, none of the patients had an eschar.
The previous studies corroborate with our findings of unfavourable outcomes in the form of preterm birth, spontaneous abortion, foetal loss, oligohydramnios and low birth weight babies (Meena et al. Citation2016). The serological method such as IgM-based ELISA is a reliable method for the detection of acute infection due to scrub typhus with good sensitivity and specificity. The IgM antibodies to O. tsutsugamushi infection are detected 1 week after infection; false negatives occur when tested before the end of one week. Molecular based methods such as polymerase chain reaction (PCR) have good diagnostic accuracy and can detect the scrub typhus even in early phase, unlike immune based methods. The major disadvantage of the serological method is the lack of standardisation and the reference method to compare the ELISA. To improve the diagnostic accuracy of the IgM ELISA, further research will be required to determine the region specific cut-offs, i.e. epidemiological cut-off (Kala et al. Citation2020). Doxycycline remains the mainstay of treatment for scrub typhus-affected patients. However, doxycycline, a class D drug, is contraindicated in pregnant women due to its teratogenic effects on the foetus (Mathai et al. Citation2003). That is why doxycycline 100 mg twice daily was administered in females presenting after delivery and post abortion. Tablet azithromycin, 500 mg once daily for seven days was given to pregnant women presenting in their antenatal period (Kim et al. Citation2006). As it effectively penetrates polymorphonuclear neutrophils and macrophages, which are target cells for Orientia tsutsugamushi, azithromycin appears to be an effective scrub typhus treatment (Alvarez-Elcoro and Enzler Citation1999). Despite receiving the prescribed medication, four (14.8%) women had poor foetal outcome and maternal death occurred in one (3.7%) patient (Chrispal et al. Citation2010). Mostly, patients were managed well in time. While, eight (29.6%) patients required intensive care facility. Since scrub typhus can impart significant burden on pregnancy outcomes, increased physician awareness is needed to reduce foetal loss among pregnant women with scrub typhus since this study shows that early identification and treatment can prevent foetal death.
Limitations
In the present study, the diagnosis of scrub typhus was based on IgM ELISA only. Since scrub IgM can be positive for many weeks, a convalescence IgM testing should also have been done. A positive scrub IgM test cannot differentiate between an acute infection and the past infection. Ideally PCR should have been done in all the cases presenting within 1 week of the fever for early-stage diagnosis of scrub typhus.
Conclusions
In conclusion, present study was a retrospective in which foetal and maternal outcome in scrub typhus positive pregnant women was analysed. Poor foetal and maternal outcomes were observed in four (14.8%) and one (3.7%) cases, respectively. Scrub typhus should be included in the differential diagnosis of AUFI in pregnant women who reside in endemic regions or have returned from one. In endemic locations, a strong index of suspicion for scrub typhus is necessary for pregnant patients with fever. The key to reduce morbidity and mortality in both the mother and the foetus is early identification and treatment. Although scrub typhus is rare in pregnancy, it needs special attention owing to possible unfavourable pregnancy outcome.
Ethics statement
We have taken ethical clearance from “Institutional Ethics Committee.”
Author contributions
Dr Bhavana Yadav – protocol design, data collection, data analysis and manuscript writing.
Dr Ranu Soni – data collection or management, data analysis and manuscript writing/editing.
Dr Manisha Biswal – data analysis and manuscript editing.
Dr Vanita Suri – data analysis and review, manuscript editing.
Dr Minakshi Rohilla – data analysis and review, manuscript editing.
Disclosure statement
The authors declare that they have no conflict of interest.
References
- Alvarez-Elcoro, S. and Enzler, M.J., 1999. The macrolides: erythromycin, clarithromycin, and azithromycin. Mayo Clinic Proceedings, 74 (6), 613–634.
- Bhat, N.K., et al., 2014. Scrub typhus in children at a tertiary hospital in north India: clinical profile and complications. Iranian Journal of Pediatrics, 24 (4), 387.
- Chrispal, A., et al., 2010. Acute undifferentiated febrile illness in adult hospitalized patients: the disease spectrum and diagnostic predictors – an experience from a tertiary care hospital in South India. Tropical Doctor, 40 (4), 230–234.
- Chrispal, A., et al., 2010. Scrub typhus: an unrecognized threat in South India – clinical profile and predictors of mortality. Tropical Doctor, 40 (3), 129–133.
- Elliott, I., et al., 2019. Scrub typhus ecology: a systematic review of Orientia in vectors and hosts. Parasites & Vectors, 12 (1), 1–36.
- Gaba, S., et al., 2020. Scrub typhus leading to acute liver failure in a pregnant patient. Cureus, 12 (9), e10191.
- Jensenius, M., Fournier, P.E. and Raoult, D., 2004. Tick-borne rickettsioses in international travellers. International Journal of Infectious Diseases, 8 (3), 139–146.
- Kala, D., et al., 2020. Diagnosis of scrub typhus: recent advancements and challenges. 3 Biotech, 10 (9), 1–21.
- Kim, Y.S., et al., 2006. Scrub typhus during pregnancy and its treatment: a case series and review of the literature. American Journal of Tropical Medicine and Hygiene, 75 (5), 955–959.
- Lakshmi, R.M.M.V.N., et al., 2020. Prevalence of scrub typhus in a tertiary care centre in Telangana, South India. Iranian Journal of Microbiology, 12 (3), 204.
- Mahajan, S.K., 2005. Scrub typhus. JAPI, 53 (955), 269.
- Mathai, E., et al., 2003. Case reports: scrub typhus during pregnancy in India. Transactions of the Royal Society of Tropical Medicine and Hygiene, 97 (5), 570–572.
- McCrumb, F. R., et al., 1957. Leptospirosis in Malaya. I. Sporadic cases among military and civilian personnel. American Journal of Tropical Medicine and Hygiene, 6 (2), 238–256.
- Meena, M., et al., 2016. Scrub typhus in pregnancy: a case series. Tropical Doctor, 46 (3), 153–156.
- Oberoi, A. and Varghese, S.R., 2014. Scrub typhus—an emerging entity: a study from a tertiary care hospital in North India. Indian Journal of Public Health, 58 (4), 281–283.
- Peter, J.V., et al., 2015. Severe scrub typhus infection: clinical features, diagnostic challenges and management. World Journal of Critical Care Medicine, 4 (3), 244–250.
- Phupong, V. and Srettakraikul, K., 2004. Scrub typhus during pregnancy: a case report and review of the literature. Southeast Asian Journal of Tropical Medicine and Public Health, 35 (2), 358–360.
- Rajan, S.J., Sathyendra, S., and Mathuram, A.J., 2016. Scrub typhus in pregnancy: maternal and fetal outcomes. Obstetric Medicine, 9 (4), 164–166.
- Sivarajan, S., et al., 2016. Clinical and paraclinical profile, and predictors of outcome in 90 cases of scrub typhus, Meghalaya, India. Infectious Diseases of Poverty, 5 (1), 47–56.
- Tseng, B.Y., et al., 2008. Immunohistochemical study of scrub typhus: a report of two cases. Kaohsiung Journal of Medical Sciences, 24 (2), 92–98.
- Watt, G., et al., 1999. Azithromycin activities against Orientia tsutsugamushi strains isolated in cases of scrub typhus in Northern Thailand. Antimicrobial Agents and Chemotherapy, 43 (11), 2817–2818.
- World Health Organization, 2012. WHO Recommended Surveillance Standards (WHO/CDS/CSR/ISR/99.2). Available at: http://data.unaids. org/Publications/IRC-pub04/surveillancestandards_en.pdf.
- Xu, G., et al., 2017. A review of the global epidemiology of scrub typhus. PLoS Neglected Tropical Diseases, 11 (11), e0006062.