

Introduction
The vaginal cuff comprises the reconstructed pericervical ring during hysterectomy. Vaginal cuff dehiscence (VCD) serves as an emergency complication of hysterectomy, with the potential for evisceration and additional morbidity (Nezhat et al. Citation2018). Most VCD occurs shortly after a hysterectomy with vaginal trauma, such as coitus and falling down (Hur et al. Citation2007). Even though extremely rare, there is still a risk of VCD long after hysterectomy, particularly for postmenopausal women with vault prolapse, which is often ignored by gynaecologists. Early Identification of high-risk individuals and offering prompt treatments can reduce the prevalence of late-onset VCD.
Here, we demonstrate a case of spontaneous VCD and emergency care in a patient with combined vaginal vault prolapse five years after hysterectomy, attempting to serve as a reference point for peers with a similar circumstance.
Case report
A 59-year-old woman presented to the emergency department (ED) with a complaint of a protrusion of bowel loops through the vagina while urinating. Five years earlier, she underwent a laparoscopic hysterectomy with bilateral salpingo-oophorectomy because of endometrial cancer, followed by 6 cycles of chemotherapy with 21 days per cycle. She reported a history of a prolapse of her vaginal vault during the last two years without treatment. In addition to endometrial cancer, she underwent transabdominal hemicolectomy for colon cancer twice and radical mastectomy for right and left breast successively, oral letrozole was taken until now. Combining genetic detection results and family history, she was diagnosed with Lynch syndrome. Three decades ago, she gave birth to a girl vaginally.
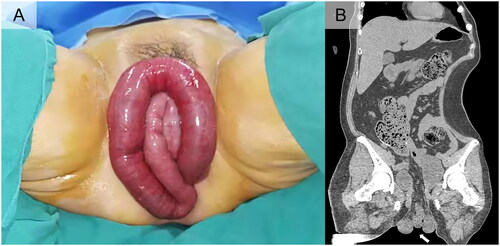
Two hours after the protrusion, she underwent a physical examination. Her vital signs were normal, and she measured 162 cm and weighed 57 kg. Cardiopulmonary examination revealed no abnormalities, and the abdomen was soft with slight tenderness and negative shifting dullness. The hypoactive bowel sounds were two times per minute by auscultation, accompanied by the absence of anal exhaust. The gynaecologic examination revealed 30 cm of small bowel emerging from the vagina. The eviscerated bowel was intact, 20 cm of which was dilatated and oedematous, with a dark red hyperaemia appearance but no signs of necrosis (). Laboratory results were in the range of normal except for a neutrophil ratio of 82.5%. Abdominal and pelvic computed tomography (CT) plain scans suggested vaginal cuff, the 5th group of small intestine and mesentery prolapse ().
Figure 1. (A) Small intestine protruding from the vagina before operation. (B) The coronal section of the plain CT scan of the pelvis and abdomen (the white arrow indicated the protruded small intestine).
Attempts of transvaginal reduction failed due to severe bowel dilatation, and urgent surgery was recommended. An open surgery via a median lower abdominal incision (20 cm) was chosen, no tumour lesions were found in the exploration, and the small intestine was returned to the abdominal cavity through the pelvic floor defect. After observing for a few minutes, the colour of the bowel returned to pink with normal peristalsis. Transvaginal cuff closure was performed using braided delayed absorbable sutures in a running, locking fashion. After the stump was closed, the vaginal vault prolapsed (POP-Q stage IV, point C = TVL= +4 cm) with atrophied vaginal mucosa. To correct the prolapse, high uterosacral ligament suspension was performed through the abdomen, and part of the rectal ligament was dissociated to suture and strengthen the pelvic floor defect. The estimated blood loss was 10 mL, and the primary challenges of the procedure were choosing the best VCD repair technique according to the patient’s situation, restoring the pelvic floor’s supportive structure, and avoiding a recurrence of vault prolapse.
The patient had her first flatus on postoperative day 1 and was discharged 9 days after her surgery. At the one-year follow-up postoperatively, there was no recurrence of vaginal prolapse.
Discussion
VCD with evisceration mainly occurs in women with a history of hysterectomy or postmenopausal prolapse. The incidence of VCD after hysterectomy is not too high, ranging from 0.14 to 4.1%, with a lower associated evisceration rate (0.032–1.2%) (Iaco et al. Citation2006, Hur et al. Citation2007, Kho et al. Citation2009). There is a strong possibility that a lasting prolapse of the vaginal vault, along with risk factors such as laparoscopic surgery, advanced age, history of operations for malignant tumours, which eventually lead to cuff dehiscence and evisceration in our case.
In most of the published cases, VCD occurred soon after the primary surgery, and the mean time varied between 6.1 weeks and 1.6 years (Cronin et al. Citation2012), only few studies have reported such cases more than five years after hysterectomy (Moen et al. Citation2003, Mastrolia et al. Citation2014, Ben Safta et al. Citation2017). In the present case, it might be possible to dehisce without additional external force because of the weak support structure of the pelvic floor and prolapsed vault while rubbing against clothing. In the case of pelvic organ prolapse, the normal vector of the vagina is shifted, stretching the already atrophic vagina even further and making it more susceptible to rupture with increasing intraabdominal pressure (Nezhat et al. Citation2018). Otherwise, oestrogen applied postoperatively has also been seen to show benefits in vaginal healing, as well as reduce the risk of VCD (Hur et al. Citation2016). In contrast, the present patient suffered a low oestrogen state under the dual influence of menopause and antiestrogen drugs postoperatively, leading to poor healing of vaginal tissue and an increased risk of vaginal prolapse.
The main clinical manifestations of VCD are abdominal and pelvic pain, vaginal bleeding and discharge; however, the diagnosis is easy to make when evisceration is present (Cronin et al. Citation2012). Once the definitive diagnosis is confirmed, surgical restoration and repair as soon as possible is preferred to prevent ischaemic necrosis of prolapsed organs. In terms of the surgical approach, exploratory laparotomy is traditionally preferred. The abdominal approach offers accurate viscus evaluation in addition to other surgical procedures, such as bowel resection. However, regarding the patients without signs of peritonitis and ischaemia of the prolapsed bowel, the transvaginal approach is equally suitable (Matthews and Kenton Citation2014).
Ideally, pelvic organ prolapse should be repaired at the time of initial hysterectomy to reduce the risk of vaginal vault prolapse. In addition to the traditional McCall culdoplasty, duplication of the uterosacral ligaments during laparoscopic hysterectomy can effectively prevent vaginal vault prolapse following surgery (Serati et al. Citation2020). For the patients with second recursion of vaginal vault prolapse, transvaginal bilateral sacrospinous fixation is an effective surgical method, which can significantly improve the quality of life and sexuality (Vitale et al. Citation2018). However, additional measures should be performed to reinforce vaginal cuff once VCD has occurred. During the present case, the rectal lateral ligament was used to reinforce the original weak tissue. In addition, tissues which were used to reinforce vaginal cuff include the pubocervical fascia, the rectovaginal fascia, omental flap, polyglactin mesh, as well as the anterior and posterior vaginal walls (Narducci et al. Citation2003, Hur et al. Citation2016, Ben Safta et al. Citation2017).
Ethical approval
This study was approved by the Ethics Committee of Peking University First Hospital prior to the commencement of the study. The study was conducted according to the principles of the Declaration of Helsinki and its amendments. Written informed consent was obtained from the individual for the publication of any potentially identifiable images or data included in this article.
Disclosure statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest. No potential conflict of interest was reported by the author(s).
References
- Ben Safta, Y., et al., 2017. Vaginal cuff dehiscence and evisceration 11 years after a radical hysterectomy: a case report. International Journal of Surgery Case Reports, 41, 234–237.
- Cronin, B., Sung, V.W., and Matteson, K.A., 2012. Vaginal cuff dehiscence: risk factors and management. American Journal of Obstetrics and Gynecology, 206 (4), 284–288.
- Hur, H.C., et al., 2007. Incidence and patient characteristics of vaginal cuff dehiscence after different modes of hysterectomies. Journal of Minimally Invasive Gynecology, 14 (3), 311–317.
- Hur, H.C., et al., 2016. Vaginal cuff dehiscence and evisceration: a review of the literature. Current Opinion in Obstetrics & Gynecology, 28 (4), 297–303.
- Iaco, P.D., et al., 2006. Transvaginal evisceration after hysterectomy: is vaginal cuff closure associated with a reduced risk? European Journal of Obstetrics, Gynecology, and Reproductive Biology, 125 (1), 134–138.
- Kho, R.M., et al., 2009. Incidence and characteristics of patients with vaginal cuff dehiscence after robotic procedures. Obstetrics and Gynecology, 114 (2 Pt 1), 231–235.
- Mastrolia, S.A., et al., 2014. Vaginal treatment of vaginal cuff dehiscence with visceral loop prolapse: a new challenge in reparative vaginal surgery? Case Reports in Obstetrics and Gynecology, 2014, 257398.
- Matthews, C.A. and Kenton, K., 2014. Treatment of vaginal cuff evisceration. Obstetrics and Gynecology, 124 (4), 705–708.
- Moen, M.D., Desai, M., and Sulkowski, R., 2003. Vaginal evisceration managed by transvaginal bowel resection and vaginal repair. International Urogynecology Journal and Pelvic Floor Dysfunction, 14 (3), 218–220.
- Narducci, F., et al., 2003. Vaginal evisceration after hysterectomy: the repair by a laparoscopic and vaginal approach with a omental flap. Gynecologic Oncology, 89 (3), 549–551.
- Nezhat, C., et al., 2018. Vaginal cuff dehiscence and evisceration: a review. Obstetrics and Gynecology, 132 (4), 972–985.
- Serati, M., et al., 2020. Laparoscopic duplication of the uterosacral ligaments following hysterectomy for stage III–IV apical pelvic organ prolapse. Updates in Surgery, 72 (1), 199–204.
- Vitale, S.G., et al., 2018. Transvaginal bilateral sacrospinous fixation after second recurrence of vaginal vault prolapse: efficacy and impact on quality of life and sexuality. BioMed Research International, 2018, 5727165.