

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Aberrant Septin9 methylation in cervical cancer has been rarely studied. We aimed to identify its diagnostic value in cervical cancer using cervical scrapings, and its predictive potential in plasma for pelvic nodal metastasis of cervical cancer. The statuses of methylated Septin9 in fresh cervical lesions and cervical scrapings were first evaluated by using quantitative methylation-specific PCR. Subsequently, the relationship between Septin9 methylation in 113 plasma samples and pelvic nodal metastasis of cervical cancer was evaluated. Methylated Septin9 was detected in all cancerous tissues, but not in cervicitis. The degrees of Septin9 methylation increased with growing severity of cervical lesions in cervical scrapings. The sensitivity of methylated Septin9 was lower than that of cytology, while it yielded a high specificity and area under the curve in detecting high-grade squamous intraepithelial lesion or cervical cancer; and when Septin9 methylation combined with HPV16/18 genotyping, the sensitivity would increase from 70.42% to 82.39%. Plasma-based Septin9 methylation had a high discriminatory power in predicting pelvic nodal metastasis of cervical cancer, with an optimal specificity of 81.48%. In conclusion, we demonstrated methylated Septin9 to be an innovative diagnostic biomarker for cervical cancer and its non-invasive predictive potential in plasma for pelvic nodal metastasis of cervical cancer.
What is already known on this subject? The occurrence of cervical cancer is related to Septin9 methylation. In fresh specimens and cervical scrapings, we found the degrees of methylated Septin9 increased with growing severity of cervical lesions. Compared with HPV16/18 genotyping and cytological detection, Septin9 methylation had a better specificity and AUC in detecting ≥ HSIL. Furthermore, plasma-based Septin9 methylation also had a high specificity for pelvic lymphatic metastasis prediction.
What the results of this study add? Methylation analysis of Septin9 indicated a similar sensitivity, specificity and AUC in detecting ≥ HSIL, relative to HPV16/18 genotyping. Compared with cytological method, Septin9 methylation also yielded a higher specificity and AUC in detecting ≥ HSIL. And we also found plasma-based Septin9 methylation had a high discriminatory power in predicting pelvic nodal metastasis of cervical cancer, with an optimal specificity of 81.48%; additionally an increasing sensitivity from 50% to nearly 80% was found when combined with SCCAg.
What the implications are of these findings for clinical practice and/or further research? This study aimed to evaluate the relationship between Septin9 methylation and cervical cancer, and to explore the value of methylated Septin9 in the detection of cervical (pre)cancerous lesions. Moreover, we would explore plasma-based ctDNA biomarkers for pelvic lymphatic metastasis prediction of cervical cancer, to improve non-invasive predictive accuracy of pelvic nodal metastasis and reduce the complications caused by pelvic lymphadenectomy.
Impact statement
1. Introduction
Cervical cancer ranks as the fourth most common gynaecologic malignancy and the fourth leading cause of cancer deaths among women worldwide, posing a serious threat to women’s health (Bray et al. Citation2018). Although cytologic and HPV-DNA tests have become available for cervical cancer screening, a substantial number of (pre)cancerous lesions have been missed for modest sensitivity of cytology; and result in unnecessary over-referral of colposcopy due to low specificity for CIN III or cervical cancer (≥CIN III) of HPV-DNA testing (Sahasrabuddhe et al. Citation2011). Therefore, it is important to find specific biomarkers for the detection of cervical cancer that possess a comparable sensitivity but with increased specificity. Persistent high risk human papillomavirus (hrHPV) infection is a prerequisite for the development of cervical cancer, but DNA methylation are also the key triggers of carcinogenic process. Many genes, including PAX1, SOX1, PCDHA, DCC, EPB41L3, FAM19A4 and others, have been confirmed to be hypermethylated in cervical scrapings diagnosed as CIN II or other aforementioned lesions (≥CIN II) (De Strooper et al. Citation2014; Lai et al. Citation2014; Wang et al. Citation2015; Clarke et al. Citation2017; Bonde et al. Citation2021).
The status of pelvic nodal metastasis is associated with prognosis and determines the postoperative treatment of cervical cancer (Cheng-Yen Lai et al. Citation2018). Therefore, pelvic lymphadenectomy is a standard procedure for radical hysterectomy in women with early-stage cervical cancer (stages IA to IB1), but only 10% of patients with cervical cancer have metastatic disease after surgery (Noguchi et al. Citation1987). Importantly, pelvic lymphadenectomy increases surgical complications and postoperative lymphedema (Li et al. Citation2012). Therefore, it is necessary to explore minimally invasive technologies that allow recognition of pelvic nodal metastasis. Recent studies have indicated that some methylated genes in plasma are closely associated with metastasis of cervical cancer (Zhang et al. Citation2017). Methylated Septin9 in circulating tumour DNA (ctDNA) has been widely utilised in colorectal cancer screening, diagnosis and monitoring (Sun et al. Citation2019; Lu et al. Citation2022). In addition, methylated Septin9 has proven to be a potential biomarker for several other tumours including gastroenteric cancer (Branchi et al. Citation2016; Xu et al. Citation2021), breast cancer (Marcus et al. Citation2019), lung cancer (Powrozek et al. Citation2014), liver cancer (Bannaga et al. Citation2021), head and neck squamous cell carcinoma (Schröck et al. Citation2017), pancreatic cancer (Cohen et al. Citation2017), as well as cervical cancer (Jiao et al. Citation2019), indicating Septin9 methylation is not tissue specific. Therefore, we conjectured whether ctDNA-based methylation analysis of Septin9 would provide a non-invasive approach to predicting pelvic nodal metastasis in cervical cancer.
We previously identified a significant growing FAM19A4 methylation in cervical scrapings from (pre)cancerous lesions compared with no-CIN lesions (Bu et al. Citation2018). In this research, based on these results, we further investigated the diagnostic value of Septin9 methylation in cervical cancer scrapings and its predictive accuracy of pelvic lymphatic metastasis in plasma of cervical cancer.
2. Materials and methods
2.1. Study population
2.1.1. Cervical fresh tissues and scrapings
We initially included eight cervical cancer tissues confirmed by pathology from our hospital, and corresponding controls from nine cervicitis without HPV infection. These samples were preserved by RNAstore solution (CWBiotech Company, Beijing, China) for subsequent methylation analysis.
We further recruited cervical scrapings on 1050 hrHPV-positive patients aged 20–65 years, who visited the study hospital between November 2016 and May 2018. All participants voluntarily accepted cervical HPV-DNA genotyping and cytologic tests. Samples of cervical scrapings were collected by experienced gynaecologists using a cervical cytobrush. After screening the specimens, 248 patients histologically confirmed with cervical cancer, HSIL, LSIL, or no-CIN lesions were included in the study (flowchart in Supplementary Figure 1(A)).
2.1.2. Peripheral blood of cervical cancer
In addition, peripheral blood samples from 148 patients with cervical cancer (stages IA to IIB) were collected before surgery from August 2017 to August 2018. Eventually, only 113 samples met the selection criteria and were included in our final analysis (flowchart in Supplementary Figure 1(B)). Whole blood was collected into a Cell-Free DNA Storage Tube (GenePhar Technologies Inc., Guangzhou, China) and stored for no more than 10 days at room temperature before centrifugation to isolate plasma.
We acquired the corresponding samples and complete clinical data of participants. Exclusion criteria included pregnancy, lactation, a history of hysterectomy, a history of cervical neoplasia and current or previous history of other cancers. Approval for this study was obtained from the Guangdong Women and Children Hospital Ethics Committee (reference number: 201901093). We obtained informed written consent prior to specimen collection, according to institutional guidelines.
2.2. Cervical HPV-DNA genotyping, cytologic testing and colposcopic biopsy
HPV-DNA genotyping tests were detected in the Department of Clinical Laboratory at our hospital by fluorescence quantification PCR in accordance with the manufacturer’s instructions (Kaipu Company, China). This method could identify 14 hrHPV genotypes (HPV-16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) and other low-risk HPV genotypes.
Cytologic smear specimens were prepared using a customised liquid-based cytology method—the ThinPrep Pap system—according to the manufacturer’s protocol (Hologic, MA, USA). The cytologic diagnoses were evaluated by two or more academic cytopathologists in accordance with the Bethesda 2001 criteria (Solomon et al. Citation2002).
Patients found positive for either cytology (threshold ≥ ASC-US ± hrHPV positive) or HPV16/18 would undergo colposcopy. Some patients with normal cytology or HPV testing but with suspected clinical history and signs were also referred for colposcopy. Multiple focal biopsies and/or endocervical curettage (ECC) were taken from abnormal areas of the cervix during colposcopic examinations (Bornstein et al. Citation2012). Histologic diagnosis was confirmed by two or more pathologists.
2.3. DNA isolation, DNA bisulphite modification and quantitative methylation-specific PCR
Genomic DNA from cervical scraping samples was extracted using a magnetic-bead-based DNA extraction kit (GenePhar Technologies Inc. China) and ctDNA samples in plasma were extracted using Nucleic Acid Purification/Magnetic Beads Kit (GeneShine Biotechnology Company, Shanghai, China) following the manufacturer’s recommendations. The extracted DNA was treated with bisulphite to convert unmethylated cytosine to uracil using the GS DNA Methylation Kit (GeneShine Biotechnology, China). The bisulphite-converted DNA was immediately used as a template for DNA methylation analysis.
The methylation queried in this study mapped upstream to 225–305 bp of the first exon of the Septin9 transcript isoform v2 (GenBank Access no. NM_001113493.1). The sequences of both primers and probes included CpG dinucleotides that can differentiate methylated from non-methylated DNA template. The following primer and probe sequences were used for Septin9 and the internal control ACTB gene (sequences in Table S1). DNA samples from cervical cancer tissues, normal peripheral blood and double-distilled water (ddH2O) were used as the positive control, negative control and blank control, respectively. Amplification reactions were performed in triplicate in a total volume of 20 μl that consisted of 10 μl of 2 × Premix Type reagent, 3 μl of bisulphite-converted DNA sample, 0.2 μl of 50 × Rox Reference Dye II reagent, 0.5 μl of each forward and reverse primer for Septin9 and ACTB and 0.8 μl of each probe of Septin9 and ACTB, with a final addition of distilled water to 20 μl. The quantitative methylation-specific PCR (qMS-PCR) was performed using an ABI 7500 PCR System (Life Technologies, USA) in a 96-well plate. Amplification was carried out by hot-start activation at 94 °C for 10 min, followed by 50 cycles of denaturation at 93 °C for 30 s, annealing at 56 °C for 60 s and extension at 65 °C for 30 s, with a final hold at 12 °C. Amplification results were determined by collecting the fluorescent signal to obtain the circulating threshold value (CT value) and the amplification curve of ACTB and Septin9 (amplification curve in Supplementary Figure 2). All samples had a CT value <32 for ACTB to assure good sample quality. Signal was defined as positive for Septin9 methylation if both two tests were positive among three repeated trials according to the amplification curve. Samples with a CT value > 45 for Septin9 were considered as negative results.
2.4. Statistical analyses
All statistical analyses were two tailed and performed using IBM SPSS Statistics Version 23 (IBM Corp, Armonk, NY, USA). Normally distributed continuous variables are presented as means ± SD, while non-normally distributed variables are presented as medians (). The Kruskal–Wallis H test and Mann–Whitney U tests were used for non-normally variables to calculate the differences in methylation scores between multiple categories and two categories, respectively. Chi-square tests (including correction for continuity and Fisher’s exact-probability test) with a Bonferroni correction were used for categorical variables. The Cochran–Armitage trend test was used to analyse the linear correlation between cervical lesions and Septin9 methylation. Receiver operating characteristics (ROC) analysis and area under the curve (AUC)—with corresponding 95% Wald confidence intervals (95% CI) of methylated Septin9—were performed using SPSS and Medcalc software Version 18.9.1 (Seoul, Korea). The differences in AUC of each detective method also performed by Medcalc software. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV) and Youden Index (YI) were calculated together with their corresponding 95% CIs, for outcomes of ≥ HSIL, and cervical cancer. The McNemar’ s test was used to calculate the differences of sensitivity and specificity in various detection methods. p Values <0.05 were considered statistically significant for all statistical methods.
3. Results
3.1. Comparison of Septin9 methylation in cervical scrapings with different severity of cervical lesions
In fresh tissue specimens, the methylation rates of Septin9 in cervical cancer tissues (8/8) were significantly higher than those for cervicitis tissues (0/9) (100% vs 0%, p = 4.10 × 10−5 < 0.0001).
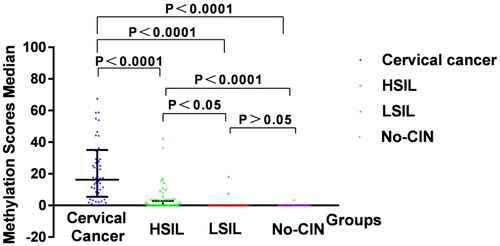
In cervical scraping samples, the Cochran–Armitage trend test showed there was a linear trend between cervical lesions and Septin9 methylation. We found Septin9 showed a clear tendency to increase methylation frequency according to the grade of cervical lesion in the no-CIN, LSIL, HSIL and cervical cancer groups, respectively (Cochran–Armitage trend test, p = 1.67 × 10−20 < 0.0001) ().
Table 1. Comparison of Septin9 methylation with different severity of cervical lesions.
The median methylation scores of the four groups tested were 1.00 × 10−3, 1.40 × 10−3, 1.77 × 10−2 and 14.07, in no-CIN, LSIL, HSIL and cervical cancer samples, respectively, with significant statistical differences across the four groups (p = 1.59 × 10−20 < 0.0001). In pairwise comparisons between groups, the median methylation scores of Septin9 in cervical cancer group and HSIL group were respectively different from other groups ( and ).
Figure 1. Methylation scores median of Septin9 with increasing severity of cervical lesions.
In this Box-and-Whisker plot, the median lines represent median values; the upper and lower lines represent the 25th and 75th percentiles, respectively.
3.2. Clinical performance indicators of Septin9 methylation, cytology (threshold ≥ ASC-US) and HPV16/18 genotyping for discrimination of cervical cancer and ≥ HSIL
Regarding the detection of cervical cancer, on one hand, Septin9 methylation had a higher sensitivity than HPV16/18 genotyping (95.52% vs 82.09%, p < 0.05); on the other hand, it had a similar sensitivity than cytologic testing and testing of HPV16/18 or Septin9 methylation, while retaining the highest specificity of 68.51%. ROC curve analysis also manifested the optimal AUC of 0.92 for Septin9 methylation in the detection of cervical cancer, with satisfactory NPV, PPV and YI ( and ).
Figure 2. The diagnostic power of Septin9 methylation, cytology and HPV16/18 genotyping.
(A) ROC of Septin9 methylation, cytology, HPV16/18 genotyping and Septin9 methylation+HPV16/18 in differentiating cervical cancer patients from non-cancerous patients.
(B) ROC of Septin9 methylation, cytology, HPV16/18 genotyping and Septin9 methylation+HPV16/18 in differentiating ≥ HSIL patients from ≤ LSIL patients.
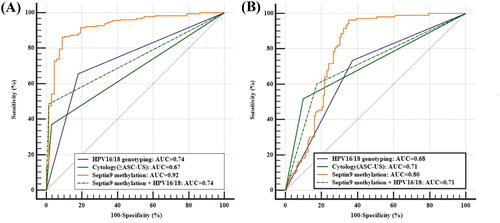
Table 2. Power of Septin9 methylation, cytology and HPV16/18 genotypin for detection ≥ HSIL and cervical cancer.
For distinguishing ≥ HSIL from ≤ LSIL, testing for methylated Septin9 had an equivalent specificity and sensitivity with testing of HPV16/18 genotyping. In addition, the sensitivity of Septin9 methylation analysis was slightly lower relative to cytologic testing and combined tests for Septin9 methylation with HPV16/18 genotyping, while the specificity was significantly higher than both of them. And these data also indicated the low sensitivity of methylated Septin9 could increase from 70.42% to 82.39%, by joint HPV16/18 genotyping testing. Overall, ROC curve analysis revealed that Septin9 methylation exhibited a strong diagnostic accuracy in discriminating ≥ HSIL from ≤ LSIL, with the highest AUC of 0.80, and a sensitivity of 70.42% and specificity of 80.19% ( and ).
3.3. Relationship between pelvic nodal metastasis of cervical cancer and Septin9 methylation in ctDNA from cervical cancer plasma
Of the 113 cervical cancer specimens, 32 patients were positive for pelvic lymph nodes (LN(+)) and 81 were negative for pelvic lymph nodes (LN(−)) as confirmed by postoperative histopathology. The average age of the 113 patients with cervical cancer was 48.08 years; and neither age, pathological type nor tumour size affected the status of pelvic nodal metastasis (p > 0.05). However, cervical cancer stage was associated with pelvic nodal metastasis, and locally advanced cervical cancer (IB2 or above) was more prone to metastasis (p < 0.05) (Supplementary Table 2).
We first defined >1.5 ng/ml as positive for SCC-Ag based on the laboratory of our hospital. Our study found no significant difference in the positive rates of SCC-Ag (threshold, 1.5 ng/ml) between the LN(+) and LN(–) groups (65.62% vs 53.09%, p > 0.05). However, the Septin9 methylation frequency in the LN(+) group was higher than that in the LN(–) group (50% vs 18.52%, P < 0.05) (Supplementary Table 3).
When we evaluated the effects of Septin9 methylation and SCC-Ag on the status of pelvic nodal metastasis by logistic regression analysis, we found that the regression model was statistically significant (p < 0.05). When two independent variables, such as SCC-Ag (positive or negative) and Septin9 methylation (yes or no) included, only Septin9 methylation status was found to be meaningful for the prediction of pelvic nodal metastasis. The OR value suggested that the risk of pelvic nodal metastasis in patients with methylated Septin9 was 4.193 times (95% CI, 2.27–12.85) than that without methylation (p < 0.05).
Septin9 methylation possessed a sensitivity equal to that of SCC-Ag in predicting pelvic nodal metastasis (50.00% vs 65.63%, p > 0.05), but a higher specificity (81.48% vs 46.91%, p < 0.05). A co-test of methylated Septin9 with SCC-Ag was utilised to improve the sensitivity in differentiating LN(+) patients from LN(–) patients, and we acquired an increasing sensitivity from 50% to nearly 80%. In addition, Septin9 methylation was also equivalent to an AUC of 0.66 when comparing all the three testing (p > 0.05) ().
Table 3. Power of Septin9 methylation in plasma and SCC-Ag for prediction of pelvic nodal metastasis.
4. Discussion
Septin9 is a novel tumour biomarker and a member of the Septin gene family involved in cell division, migration, apoptosis and DNA repair (Connolly et al. Citation2011). A recent study found that Septin9 was hypermethylated in cervical cancer tissues compared to the normal controls, with satisfactory sensitivity and specificity (Jiao et al. Citation2019). However, the feasibility of detecting Septin9 methylation in cervical scrapings has not yet been carried out. Our team previously established a high-quality qMS-PCR methylation method for non-invasive screening of colorectal cancer. In our pilot study, we also found Septin9 transcript isoform v2 was highly methylated in cervical cancer tissues. We further confirmed that in cervical scrapings, increases in Septin9 methylation were significantly correlated with greater severity of cervical lesions, which was consistent with Jiao’s recent report (Jiao et al. Citation2019). This study revealed a slightly poor sensitivity of methylated Septin9 in identifying ≥ HSIL than cytologic testing (70.42% vs 90.14%), while displayed a superior specificity (80.19% vs 51.89%), with a correspondingly equivalent AUC (0.80 vs 0.71). These data were similar with our previous work that methylated FAM19A4 had a lower sensitivity but higher specificity than cytologic testing in detecting ≥ HSIL (Bu et al. Citation2018). In brief, although Septin9 methylation showed a slightly poorer sensitivity in detecting ≥ HSIL, it still played an indispensable role in detecting cervical cancer. Septin9 methylation testing can reduce the rates of excessive colposcopy referral and over-diagnosis in clinical application; and improve the accuracy of detection rates of cervical lesions for its high specificity.
This study explored Septin9 methylation in HPV-positive patients, while HPV-negative patients were not mentioned. However, more and more studies have found that HPV-negative cervical cancer, which may be caused by low-risk HPV carcinogenesis, “Hit and Run Theory”, and sampling errors or laboratory errors (Macios and Nowakowski Citation2022), suggesting hr-HPV detection alone may miss 10–15% ≥HSIL lesions. This study indicated the detection rate of Septin9 methylation in cervical cancer scrapings was as high as 95.52%, and in ≥ HSIL lesions was 70.42%. This suggested hr-HPV and methylation joint testing were more conducive to disease risk assessment, reducing missed diagnosis of cervical cancer. After 5 years of follow-up, some scholars found that ≥ HSIL patients with HPV-negative had less recurrence than HPV-positive patients (Bogani et al. Citation2021). Furthermore, a long-term follow-up study indicated that the cervical cells showing FAM19A4/mir124-2 methylation had a remarkable tendency to progress to cancer (De Strooper et al. Citation2018), which was similar to Dick’s (Citation2019) research that FAM19A4/miR124-2 methylation-positive women had a much higher 14 year risk of CIN3+ than those negative women. Another review also raised an argument that an absence of methylation in HSIL did not progress (Lorincz Citation2016), and methylation-negative patients with untreated CIN2+ had more disease regression than methylation-positive patients (Kremer et al. Citation2022). In conclusion, we speculated that cervical lesions with HPV-negative and methylation-negative would progress at a low risk. However, it needs to be confirmed by further prospective studies. We also herein explored for the first time the role of methylated Septin9 in plasma for the prediction of cervical cancerous pelvic nodal metastasis. Some studies have depicted a 5-year survival rate for patients without lymph node metastasis of 85–90%, which then declined to 50–55% with lymph node metastasis, suggesting a vital role for the latter in the prognosis of cervical cancer (Thaker et al. Citation2015). Preoperative magnetic resonance (MR) examination was often used to determine the presence of pelvic metastatic lymph nodes for cervical cancer, and the criteria for MR diagnosis was the maximal axial diameter of more than 10 mm. However, reviews displayed a varying sensitivity of 0.38–0.89 and specificity of 0.78–0.99 for MR imaging (Reinhardt et al. Citation2001), and MR imaging technology was expensive and patients with MR contraindications could not perform MR examination. Hence, attention has shifted to the application of serum-based biomarkers recently. The serum-based protein biomarker SCC-Ag has been commonly used for evaluating the status and prognosis of cervical cancer, whereas such proteins can also be found at low concentrations in individuals without cancer (Dasari et al. Citation2015). Nevertheless, tumour markers in ctDNA do not occur in non-neoplastic diseases, and higher levels of ctDNA can be detected in over 80% of metastatic tumours—more than is observed for most conventional biomarkers (Diehl et al. Citation2005; Bettegowda et al. Citation2014). Therefore, plasma-based ctDNA detection as a non-invasive examination of solid tumours (termed ‘liquid-biopsy’) has provided an alternative to tissue-biopsy, reducing the pain, risk and expense caused by tissue biopsy.
Our study revealed that both Septin9 methylation and SCC-Ag effectively reflected the status of lymph node metastasis of cervical cancer. Furthermore, we calculated the optimal SCC-Ag threshold (3.8 ng/ml) to predict the status of pelvic nodal metastasis, consistent with the findings by Takeshima and Xu (Takeshima et al. Citation1998; Xu et al. Citation2018) where the optimal SCC-Ag thresholds were 4 and 3.26 ng/ml. Although Septin9 methylation was less sensitive than SCC-Ag, the former manifested the greatest specificity at 81.48% and a PPV of 51.61%, which would predict nodal metastasis more accurately. In addition, we also demonstrated that the co-test of methylated Septin9 and SCC-Ag was more sensitive in the identification of lymph node metastasis. In clinical application, the satisfactory specificity of methylated Septin9 made it an accurate and reliable method of defining patients at high risk for pelvic lymphatic metastasis. When SCC-Ag was coupled to Septin9 methylation, the combination was more sensitive in recognising lymph node metastasis.
In conclusions, we herein report the relationship between Septin9 methylation and cervical cancer. In addition, we are the first to apply a plasma-based Septin9 methylation as a biomarker to predict pelvic nodal metastasis of cervical cancer, providing a foundation for the future development of non-invasive follow-up of cervical cancer. Nevertheless, there is a limitation of this study that this is a retrospective study, and the relative scarcity of long-term follow-up data makes untenable the analysis of methylated Septin9 in predicting progression of benign cervical lesions to cervical cancer. Thus, a larger number of specimens, follow-up analysis and prospective experiments are required to verify the prognostic performance of Septin9 methylation.
Ethical approval
All patients provided informed consent and agreed to participate in the study. The present study was approved by the Guangdong Women and Children Hospital Ethics Committee (reference number 201901093).
Consent to participate statement
All participants gave written informed consent.
Supplemental Material
Download MS Word (268.6 KB)Acknowledgements
We thank all the participants who took part in these trials and contributed to this research. We thank GeneShine Biotechnology in China for the help of qMS-PCR detection technology. We thank LetPub (www.letpub.com) for its linguistic assistance during the preparation of this manuscript.
Disclosure statement
The author(s) indicated no potential conflicts of interest related to this article.
Data availability statement
According to Norwegian data legislation, the data of this study cannot be made generally available. Requests should be sent to the corresponding author.
Additional information
Funding
References
- Bannaga, A.S., et al., 2021. Role of methylated septin 9 as an adjunct diagnostic and prognostic biomarker in hepatocellular carcinoma. HPB (Oxford), 23 (10), 1595–1606.
- Bettegowda, C., et al., 2014. Detection of circulating tumor DNA in early- and late-stage human malignancies. Science Translational Medicine, 6 (224), 224r.
- Bogani, G., et al., 2021. High-risk HPV-positive and -negative high-grade cervical dysplasia: Analysis of 5-year outcomes. Gynecologic Oncology, 161 (1), 173–178.
- Bonde, J., et al., 2021. Methylation markers FAM19A4 and miR124-2 as triage strategy for primary human papillomavirus screen positive women: A large European multicenter study. International Journal of Cancer, 148 (2), 396–405.
- Bornstein, J., et al., 2012. 2011 colposcopic terminology of the International Federation for Cervical Pathology and Colposcopy. Obstetrics and Gynecology, 120 (1), 166–172.
- Branchi, V., et al., 2016. Promoter hypermethylation of SHOX2 and SEPT9 is a potential biomarker for minimally invasive diagnosis in adenocarcinomas of the biliary tract. Clinical Epigenetics, 8, 133.
- Bray, F., et al., 2018. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 68 (6), 394–424.
- Bu, Q., et al., 2018. The clinical significance of FAM19A4 methylation in high-risk HPV-positive cervical samples for the detection of cervical (pre)cancer in Chinese women. BMC Cancer, 18 (1), 1182.
- Cheng-Yen Lai, J., et al., 2018. The role of sentinel lymph node biopsy in early-stage cervical cancer: A systematic review. Taiwanese Journal of Obstetrics & Gynecology, 57 (5), 627–635.
- Clarke, M.A., et al., 2017. Discovery and validation of candidate host DNA methylation markers for detection of cervical precancer and cancer. International Journal of Cancer, 141 (4), 701–710.
- Cohen, J.D., et al., 2017. Combined circulating tumor DNA and protein biomarker-based liquid biopsy for the earlier detection of pancreatic cancers. Proceedings of the National Academy of Sciences of the United States of America, 114 (38), 10202–10207.
- Connolly, D., et al., 2011. Septin roles in tumorigenesis. Biological Chemistry, 392 (8–9), 725–738.
- Dasari, S., Wudayagiri, R. and Valluru, L., 2015. Cervical cancer: Biomarkers for diagnosis and treatment. Clinica Chimica Acta: International Journal of Clinical Chemistry, 445, 7–11.
- De Strooper, L., et al., 2018. Cervical cancer risk in HPV-positive women after a negative FAM19A4/mir124-2 methylation test: A post hoc analysis in the POBASCAM trial with 14 year follow-up. International Journal of Cancer, 143 (6), 1541–1548.
- De Strooper, L.M., et al., 2014. Methylation analysis of the FAM19A4 gene in cervical scrapes is highly efficient in detecting cervical carcinomas and advanced CIN2/3 lesions. Cancer Prevention Research (Philadelphia, PA), 7 (12), 1251–1257.
- Dick, S., et al., 2019. Long-term CIN3+ risk of HPV positive women after triage with FAM19A4/miR124-2 methylation analysis. Gynecologic Oncology, 154 (2), 368–373.
- Diehl, F., et al., 2005. Detection and quantification of mutations in the plasma of patients with colorectal tumors. Proceedings of the National Academy of Sciences of the United States of America, 102 (45), 16368–16373.
- Jiao, X., et al., 2019. Promoter methylation of SEPT9 as a potential biomarker for early detection of cervical cancer and its overexpression predicts radioresistance. Clinical Epigenetics, 11 (1), 120.
- Kremer, W.W., et al., 2022. Clinical regression of high-grade cervical intraepithelial neoplasia is associated with absence of FAM19A4/miR124-2 DNA methylation (CONCERVE study). Journal of Clinical Oncology: Official Journal of the American Society of Clinical Oncology, 40 (26), 3037–3046.
- Lai, H.C., et al., 2014. PAX1/SOX1 DNA methylation and cervical neoplasia detection: a Taiwanese Gynecologic Oncology Group (TGOG) study. Cancer Medicine, 3 (4), 1062–1074.
- Li, D., et al., 2012. Surgical-pathologic risk factors of pelvic lymph node metastasis in stage Ib1-IIb cervical cancer. Acta Obstetricia et Gynecologica Scandinavica, 91 (7), 802–809.
- Lorincz, A.T., 2016. Virtues and weaknesses of DNA methylation as a test for cervical cancer prevention. Acta Cytologica, 60 (6), 501–512.
- Lu, P., et al., 2022. Methylated septin 9 as a promising biomarker in the diagnosis and recurrence monitoring of colorectal cancer. Disease Markers, 2022, 7087885.
- Macios, A. and Nowakowski, A., 2022. False negative results in cervical cancer screening-risks, reasons and implications for clinical practice and public health. Diagnostics, 12 (6), 1508.
- Marcus, J., et al., 2019. Septin 9 isoforms promote tumorigenesis in mammary epithelial cells by increasing migration and ECM degradation through metalloproteinase secretion at focal adhesions. Oncogene, 38 (30), 5839–5859.
- Noguchi, H., et al., 1987. Pelvic lymph node metastasis of uterine cervical cancer. Gynecologic Oncology, 27 (2), 150–158.
- Powrozek, T., et al., 2014. Septin 9 promoter region methylation in free circulating DNA-potential role in noninvasive diagnosis of lung cancer: preliminary report. Medical Oncology (Northwood, London, England), 31 (4), 917.
- Reinhardt, M.J., et al., 2001. Metastatic lymph nodes in patients with cervical cancer: detection with MR imaging and FDG PET. Radiology, 218 (3), 776–782.
- Sahasrabuddhe, V.V., Luhn, P. and Wentzensen, N., 2011. Human papillomavirus and cervical cancer: biomarkers for improved prevention efforts. Future Microbiology, 6 (9), 1083–1098.
- Schröck, A., et al., 2017. Free-circulating methylated DNA in blood for diagnosis, staging, prognosis, and monitoring of head and neck squamous cell carcinoma patients: an observational prospective cohort study. Clinical Chemistry, 63 (7), 1288–1296.
- Solomon, D., et al., 2002. The 2001 Bethesda System: terminology for reporting results of cervical cytology. JAMA, 287 (16), 2114–2119.
- Sun, J., et al., 2019. The role of (m)SEPT9 in screening, diagnosis, and recurrence monitoring of colorectal cancer. BMC Cancer, 19 (1), 450.
- Takeshima, N., et al., 1998. The value of squamous cell carcinoma antigen as a predictor of nodal metastasis in cervical cancer. Gynecologic Oncology, 68 (3), 263–266.
- Thaker, N.G., et al., 2015. Survival outcomes for patients with stage IVB vulvar cancer with grossly positive pelvic lymph nodes: time to reconsider the FIGO staging system? Gynecologic Oncology, 136 (2), 269–273.
- Wang, K.H., et al., 2015. Global methylation silencing of clustered proto-cadherin genes in cervical cancer: serving as diagnostic markers comparable to HPV. Cancer Medicine, 4 (1), 43–55.
- Xu, F., et al., 2018. Preoperative SCC-Ag and thrombocytosis as predictive markers for pelvic lymphatic metastasis of squamous cervical cancer in early FIGO stage. Journal of Cancer, 9 (9), 1660–1666.
- Xu, J., et al., 2021. A combination of methylation and protein markers is capable of detecting gastric cancer detection by combined markers. Epigenomics, 13 (19), 1557–1570.
- Zhang, J., et al., 2017. Aberrant methylation of MEG3 functions as a potential plasma-based biomarker for cervical cancer. Scientific Reports, 7 (1), 6271.