

Abstract
To assess whether post-hysterosalpingography evaluation was associated with pregnancy rate and to identify independent risk factors for pregnancy success after salpingostomy in patients with hydrosalpinx. A retrospective analysis was conducted on the clinical data of 47 patients diagnosed with hydrosalpingography (HSG) in our hospital from 2015 to 2018. These patients received laparoscopic surgery and another salpingography within 2 months after surgery. According to the fallopian tube conditions evaluated by HSG before and after surgery, the patients could be divided into two groups. According to the pregnancy rate and postoperative HSG of patients with hydrosalpinx after laparoscopy, the total pregnancy rate of the tubal improved group was 65.62%, while that of the non-improved group was 20%, with statistical significance (p < 0.05). We found that hysterosalpingography after salpingostomy in patients with hydrosalpinx can provide reference for clinical treatment and improve the prognosis of patients.
SYNOPSIS
Postoperative HSG improvement was an independent risk factor for pregnancy rate in patients with hydrosalpinx after laparoscopic surgery.
What is already known on this subject? Fallopian tube obstruction is an important cause of female infertility. Current studies have shown that most spontaneous pregnancies in patients with hydrosalpinx after salpingostomy occur within 18 months, however, pregnancy rates and outcomes vary from report to report.
What do the results of this study add? Many studies have shown that hydrosalpinx reduces the success rate of natural pregnancy and embryo transfer, but the mechanism of hydrosalpinx affecting pregnancy remains unclear. This study explored the mechanism of successful pregnancy through hysterosalpingography after salpingostomy in patients with hydrosalpinx.
What are the implications of these findings for clinical practice and/or further research? To evaluate the prognosis of patients with hydrosalpinx after laparoscopic salpingostomy by hysterosalpingography (HSG), and to reflect the improvement according to the postoperative pregnancy rate of the patients. To provide clinical personalized treatment plan.
Impact statement
Introduction
Tubal factors account for about 25% of female infertility, and hydrosalpinx is the most serious manifestation of tubal diseases, comprising 10–30% tubal diseases (Aboulghar et al. Citation1998). Hydrosalpinx is the dilation or expansion of the fallopian tube during distal tubal obstruction, and the main risk factors include pelvic inflammatory disease (PID), endometriosis, appendicitis and previous pelvic or abdominal surgery (Strandell Citation2000, Ng and Cheong Citation2019). Currently, it is admitted that infection by Chlamydia causes fallopian tube inflammation (Park et al. Citation2017), and the formation of hydrosalpinx is associated with increased inflammatory mediators, structural changes of intraciliary epithelial cilia, secretory cell hyperfunction, upregulated cystic fibrosis transmembrane conductance regulator and secretion of ovarian stimulating hormones (Ajonuma et al. Citation2002). Recently, scholars have found that altered redox homeostasis, complement activation and immune cell phagocytosis are related to the formation of hydrosalpinx (Yohannes et al. Citation2019). Multiple studies have demonstrated that hydrosalpinx formation has a negative effect on natural conception and reproductive techniques such as in-vitro fertilisation (IVF), which reduces the success rates of natural pregnancy and embryo transfer (Ajonuma et al. Citation2002, Harb et al. Citation2019, Cohen et al. Citation2018, Hong et al. Citation2018). A recent systematic review also showed that undergoing assisted fertility treatment for hydrosalpinx could increase the success rate of IVF (Xu et al. Citation2017). The mechanism by which hydrosalpinx affects pregnancy remains undefined. However, it is speculated that it may be related to embryo toxicity of hydrops, reduced endometrial receptivity and mechanical flushing of hydrops (Strandell Citation2000, Strandell and Lindhard Citation2002).
Salpingostomy is distal tubal plastic surgery to manage hydrosalpinx using scissors, electrosurgery or laser (Gomel and Wang Citation1994), with the aim of preserving the fallopian tubes and allowing the patient to attempt natural conception. During surgery, the distal tube is incised and opened in the avascular area, and the newly created ostium is sutured back to the mesosalpinx (Ng and Cheong Citation2019). However, pregnancy rates and outcomes in various reports differ (Gomel Citation2015). It is admitted that pregnancy rate and outcome are associated with patient age, tubal stage, adhesion stage, the operative technique used and infection by Chlamydia (Audebert and Pouly Citation2014). In addition, scholars have found that most natural pregnancies after salpingostomy in patients with hydrosalpinx occur within 18 months (Chu et al. Citation2015).
To date, studies assessing fallopian tube improvement after laparoscopic salpingostomy in patients with hydrosalpinx are scarce, although this could lead to better pregnancy rate and outcome. Such evaluation could be performed by hysterosalpingography (HSG), providing insights into individualised management of these patients (Juneau and Bates Citation2012, Katler et al. Citation2018). Therefore, the aim of this study was to examine whether postoperative evaluation by hysterosalpingography is associated with pregnancy rate, and to identify independent risk factors for successful pregnancy after salpingostomy in patients with hydrosalpinx.
Methods
Study population and design
This study assessed clinical data of patients with hydrosalpinx who underwent HSG both before and after laparoscopic salpingostomy in the Department of Radiology and Obstetrics and Gynaecology, the Third Affiliated Hospital of Guangzhou Medical University, from 1 January 2015 to 31 December 2018.
Inclusion criteria were: (1) failure to achieve live pregnancy for more than 1 year without contraceptive measures; (2) normal sperm examination results of their spouses/partners; (3) preoperative HSG indicating unilateral or bilateral hydrosalpinx; (4) postoperative HSG performed within 2 months; (5) clinical treatment, expecting natural pregnancy or artificial assisted reproductive technology (IVF) at least 18 months after postoperative HSG.
Exclusion criteria were: (1) congenital reproductive tract abnormalities; (2) laparoscopic findings of bilateral tubal ligation; (3) preoperative HSG suggesting tubal tuberculosis.
This study was approved by the ethics committee of the Third Affiliated Hospital of Guangzhou Medical University (No. [2019]010).
Since this was a retrospective study, informed consent was not required. However, informed consent was obtained from individual participants for publishing their images.
Diagnostic criteria and grouping
The diagnostic criteria in HSG consisted of the following (Simpson et al. Citation2006) : (1) at least partial filling of the tube; (2) swelling of the tube and without contrast in the peritoneal cavity; (3) iodised oil accumulated on the umbrella end of the oviduct;(4) no iodised oil diffused in the pelvic area ().
Figure 1. Preoperative and postoperative HSG showing fallopian tube improvement. (A) Preoperative pelvic image. (B,C) Radiography showing displayed uterine cavity; the fallopian tube was displayed to the distal end of the ampulla, with no iodised oil at the umbrella end. (D) Pelvic review image after 24 h. The iodised oil was accumulated on the umbrella end of the bilateral fallopian tubes (small white arrows), and not diffused in the pelvic cavity. (E) Pelvic image after operation. (F,G) Radiography showing the uterine cavity and the fallopian tube till the umbrella end; the iodised oil overflowed into the pelvic cavity. (H) Pelvic cavity review image showing that iodised oil was evenly distributed to the pelvic cavity 24 h later.
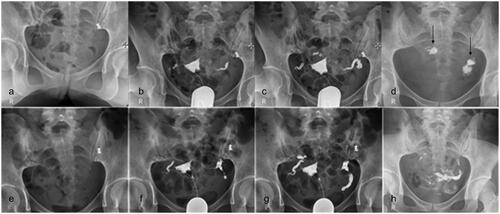
Standard for improvement of hydrosalpinx was as follows: (1) display of the whole fallopian tube; (2) no sign of hydrosalpinx at the end of the umbrella; (3) visible iodised oil into the pelvic area ().
Based on preoperative HSG and the evaluation during the laparoscopic salpingostomy, pelvic adhesion was scored as proposed by Mage et al. (Citation1986): absent, 0; mild, 1–9; moderate, 11–20; severe, 20. Meanwhile, distal tubal obstruction was also scored in accordance with the classification reported by Mage et al. (Citation1986), as follows: grade I, 2–5; grade II, 7–10; grade III, 12–15; grade IV, ≥15.
According to fallopian tube improvement assessed by preoperative and postoperative HSG, the patients could be divided into two groups (improvement and non-improvement groups), with five subgroups. (1) Unilateral hydrosalpinx with unilateral improvement and (2) bilateral hydrosalpinx with bilateral improvement groups constituted the improvement group. (3) Unilateral hydrosalpinx without improvement, (4) bilateral hydrosalpinx with unilateral improvement and (5) bilateral hydrosalpinx without improvement groups formed the non-improvement group.
HSG procedure
Examination was performed at days 7–12 of the menstrual cycle with two contraindications such as pregnancy and active pelvic infection. The patient was placed supine on the fluoroscopy table in the lithotomy position. The perineum was disinfected with povidone-iodine solution and draped with sterile towels. A speculum was inserted into the vagina and the cervix was localised and cleaned with povidone-iodine solution. A 5-F HSG catheter was positioned in the cervical canal. The balloon was inflated fully (or to the extent that the patient could tolerate). Then, a metallic marker was placed over one side of the pelvis to indicate the right or left side of the patient. A scout radiograph of the pelvis was obtained with the catheter in place before contrast material was instilled. Oil-soluble contrast material was then slowly instilled, with fluoroscopic images acquired intermittently to evaluate the uterus and fallopian tubes. Four spot radiographs after scout radiography were obtained. The first image was obtained during early filling of the uterus, while the second was acquired with the uterus fully distended. The third image was obtained to evaluate the fallopian tubes, and the fourth image should exhibit no intraperitoneal spillage of contrast agent. Finally, delayed images were acquired for 24∼ 48 h. Conventional antibiotics were used after examination and pelvic baths and coitus were prohibited within 2 weeks. Two radiologists with more than 15 years of experience in HSG diagnosis observed the images and consensually discussed to make the final diagnosis.
Surgical methods
Laparoscopic surgery was performed under the endotracheal intubation and intravenous anaesthesia by a deputy chief physician or above. The corresponding operation was performed according to the degree of adhesion between the pelvis and abdominal cavity, fallopian tube morphology and the degree of hydrosalpinx during the operation. Adhesiolysis was performed first when necessary. Then, pelvic adhesions were separated and the normal anatomical structure was restored, followed by a 1.0-cm incision in the tubal umbrella, which was with curved forceps. Surgeons clamped and everted the fallopian tube mucosa with forceps to suture and fix the fallopian tubes. To assess the patency of the fallopian tube, 10–20 ml of diluted methylene blue solution was injected through the uterine cavity, observing fallopian tube patency and taking the corresponding measures.
Observation indicators
The clinical data of patients were assessed, including preoperative and postoperative HSG images, pregnancy rate, pregnancy mode and pregnancy outcome, within 18 months.
Statistical analysis
Statistical analysis was performed with SPSS version 26.0 (IBM, Armonk, NY). Continuous data were expressed as mean ± SD. Categorical data were expressed as n (%). Categorical data were compared by the Chi-square test. Cox regression analysis was performed and variables with p < 0.05 in univariate analysis were entered into multivariable analysis. Kaplan–Meier curves were used to determine cumulative risk of pregnancy rate and risk difference was analysed by the long-rank test. p < 0.05 was considered statistically significant.
Results
Baseline characteristics of the patients
A total of 47 patients were included in this study and divided into the improvement (32 cases) and non-improvement (15 cases) groups according to the status of fallopian tube improvement, as assessed by postoperative hysterosalpingography (). There were no statistically significant differences in clinical data between the improvement and non-improvement groups (p > 0.05), except for pregnancy rate. According to postoperative HSG, there were 20 cases of pregnancy in the tubal improvement group and 3 cases in the non-improvement group. The overall pregnancy rate was 65.62% in the fallopian tube improvement group, versus 20% in the non-improvement group. The pregnancy rates in both groups were significantly different (). In addition, there were less ectopic pregnancy cases (9.52%) in the improvement group compared with the non-improvement group (33.33%). Moreover, there were 25 spontaneous pregnancies in the improvement group, natural pregnancy rate in the improvement group was 46.88%, versus 13.33% in women showing no hydrosalpinx improvement. The pregnancy rates in both groups were significantly different.
Table 1. Clinical data in both patient groups.
Cox regression analysis of factors affecting pregnancy rate
Univariate cox regression analysis showed that patient age, pelvic adhesion score, distal fallopian tube obstruction score and oviduct improvement according to postoperative HSG were associated with pregnancy in infertile patients (). Pregnancy rate in infertile patients was related to age. Specifically, pregnancy rate in women below 35 years old was significantly higher than that of older females (p < 0.10). In addition, pregnancy rate in infertile patients was related to laparoscopic pelvic adhesion and distal tubal obstruction scores. The more severe the pelvic adhesion and distal tubal obstruction, the lower the pregnancy rate. Furthermore, pregnancy rate in infertile patients was also correlated with the fallopian tube improvement status based on postoperative HSG. Indeed, pregnancy rate was significantly higher in the fallopian tube improvement group compared with the non-improvement group. According to the Kaplan–Meier method and long-rank test, average time to conception in the improvement and non-improvement groups were 12.63 (10.42–14.83) months and 15.67 (13.18–18.15) months, respectively. These findings indicated that the improvement group had higher pregnancy rate and shorter time to conception compared with the non-improvement group. Pregnancy rate curves in the improvement and non-improvement groups after salpingostomy are shown in .
Figure 2. Pregnancy curves in the oviduct improvement and non-improvement groups. The improvement group showed significantly higher cumulative pregnancy rate compared with the non-improvement group (p < 0.05).
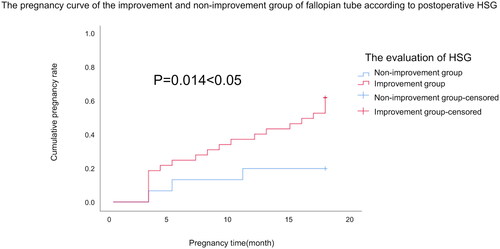
Table 2. Univariate and multivariate Cox regression analyses of pregnancy-related factors after salpingostomy.
Four factors, including age, pelvic adhesion score, distal tubal obstruction score and postoperative HSG evaluation, were filtered by univariate cox analysis and included into Cox regression multivariate analysis. The results showed that the oviduct improvement status according to postoperative HSG was an independent factor for elevated pregnancy rate in infertile patients (RR = 4.297, 95% CI: 1.225–15.07; p = 0.023), as shown in . In the improvement group, pregnancy, live birth, miscarriage and ectopic pregnancy rates were 65.62%, 66.67%, 23.80% and 9.52%, respectively; pregnancy, live birth and ectopic pregnancy rates were 20.0%, 66.67% and 33.33%, respectively, in the non-improved group.
According to fallopian tube improvement by preoperative and postoperative HSG, the patients were divided into five subgroups. Among the different subgroups, the unilateral hydrosalpinx with unilateral improvement group had the highest pregnancy rate and the best pregnancy outcome, with pregnancy and live birth rates of 66.67% and 68.75%, respectively. Detailed data are shown in .
Table 3. Pregnancy outcomes in different subgroups of patients based on fallopian tube improvement, as assessed by postoperative HSG evaluation.
Discussion
This study demonstrated that the oviduct improvement status according to postoperative HSG was an independent factor for elevated pregnancy rate in infertile patients, indicating that HSG examination should be considered for evaluating fallopian tube improvement in patients with hydrosalpinx, to provide a clinical reference for the next treatment.
As shown above, the improvement group based on HSG assessment after salpingostomy had significantly higher overall pregnancy rate compared with the non-improvement group. The higher overall pregnancy rate may be related to non-serious damage of the fallopian tube mucosa with complete function in the improvement group. In addition, diffusion of iodised oil into the pelvis through the improved distal fallopian tube may play a role. Indeed, use of oil contrast for tubal patency examination could rinse debris and remove mucus blockage from the unobstructed fallopian tube, which has a high pregnancy rate. In addition, oil contrast may affect the activity of peritoneal macrophages and endometrial receptivity, thereby enhancing fertility through implant-mediated mechanisms and increasing the pregnancy rate (Johnson et al. Citation1992, Dreyer et al. Citation2017).
Univariate analysis of potential factors affecting pregnancy revealed that pregnancy rate was associated with age, with patients below 35 years old showing a higher pregnancy rate compared with older counterparts. The negative correlation between pregnancy rate and maternal age is well known and may be affected by many influencing factors (Radoń-Pokracka et al. Citation2019, Wang et al. Citation2011). The baseline probability of female infertility is estimated at about 1%, which does not change with age. However, the actual percentage of female infertility increases with age (Dunson et al. Citation2004). Single-factor analysis also showed that pregnancy rate was related to pelvic adhesion and distal tubal obstruction scores. The higher the score and grade, the lower the pregnancy rate. This corroborated findings by Alain Audebert et al. who found that the rate of natural pregnancy after salpingostomy is associated with distal tubal obstruction and pelvic adhesion scores (Audebert and Pouly Citation2014, Singhal et al. Citation1991). This study also found that postoperative HSG assessing the hydrosalpinx improvement status was a relevant factor affecting pregnancy. Indeed, the improvement group had higher pregnancy rate and shorter time to pregnancy compared with the non-improvement group.
Cox multivariate regression analysis found that postoperative HSG showing the improvement status of the fallopian was an independent risk factor for overall pregnancy rate. The improvement group had 4.297 times higher odds of establishing pregnancy compared with the non-improvement group. Meanwhile, other factors were not significantly related to pregnancy, inconsistent with Audebert and Pouly (Citation2014). It is speculated that improvement of oviduct according to postoperative HSG may be related to the patient’s infertility duration, and pelvic adhesion and distal tubal obstruction scores, which should be verified in future large studies.
Hydrosalpinx improvement positively affects natural pregnancy and artificially assisted reproduction such as IVF, increasing the pregnancy rate and shortening the time required for pregnancy (Strandell et al. Citation2001). In this study, according to postoperative HSG, there were 20 cases of pregnancy in the tubal improvement group and 3 cases in the non-improvement group. The overall pregnancy rate was 65.62% in the fallopian tube improvement group, versus 20% in the non-improvement group, indicating a statistical significance. In addition, there were less ectopic pregnancy cases (9.52%) in the improvement group compared with the non-improvement group (33.33%). Moreover, there were 25 spontaneous pregnancies in the improvement group, natural pregnancy rate in the improvement group was 46.88%, versus 13.33% in women showing no hydrosalpinx improvement. A recent meta-analysis found that pregnancy rate in patients with hydrosalpinx after salpingectomy or proximal tubal occlusion following IVF treatment alone is 44.0%, with a live birth rate of 37.4% (Xu et al. Citation2017). Compared with the downward comprehensive treatment (natural pregnancy or ART), overall pregnancy rate in the improvement group was higher, as well as live birth rate. A study reported a natural pregnancy rate of 21.2% at 18 months after salpingostomy (95%CI: 18.6–24.1%), for a live birth rate of 25% (95%CI: 22–28%) (Chu et al. Citation2015). Compared with the above results, natural pregnancy and live birth rates in the improvement group were elevated, while pregnancy rate in the non-improvement group was reduced.
Based on fallopian tube improvement according to postoperative HSG, the patients were divided into the unilateral hydrosalpinx with unilateral improvement, bilateral hydrosalpinx with bilateral improvement, unilateral hydrosalpinx without improvement, bilateral hydrosalpinx with unilateral improvement and bilateral hydrosalpinx without improvement groups. Of these, the unilateral hydrosalpinx with unilateral improvement group had the highest pregnancy rate and the best pregnancy outcomes, followed by the bilateral hydrosalpinx with bilateral improvement and unilateral hydrosalpinx without improvement groups. There were 24 cases in the unilateral hydrosalpinx group with unilateral improvement, of which 6 cases had ART and 18 cases had natural conception. Meanwhile, overall pregnancy rates in the bilateral hydrosalpinx with unilateral improvement and bilateral hydrosalpinx without improvement groups were the lowest. These findings corroborated Jansan et al. who found significantly elevated intrauterine pregnancy rate in the unilateral hydrosalpinx group after salpingostomy compared with the bilateral hydrosalpinx group (Jansen Citation1980). The diverse pregnancy outcomes of the five different subgroups may be related to residual hydrosalpinx according to postoperative HSG examination. Based on these findings, patients with postoperative HSG suggesting fallopian tube improvement could select natural pregnancy or IVF treatment, which both result in elevated pregnancy rates and outcomes. The non-improvement group should undergo salpingectomy or proximal obstruction as soon as possible to treat the residual hydrosalpinx, improving the pregnancy rate. This was the first study to assess the effectiveness of laparoscopic salpingostomy by postoperative HSG in patients with hydrosalpinx.
This study had some limitations. First, its retrospective design carries inherent shortcomings. In addition, the sample size was relatively small, preventing subgroup analysis. Furthermore, its single-center nature may limit the generalisability of findings. Therefore, related multi-center prospective studies are warranted to confirm the present findings.
In summary, while laparoscopic salpingostomy treats hydrosalpinx, it also retains the hope of natural pregnancy for the patient, but the degree of the patient’s tubal lesions and the operator’s operating techniques would determine the effectiveness of salpingostomy. For infertile patients with hydrosalpinx, it might be a smart choice to perform HSG after laparoscopic salpingostomy to evaluate fallopian tube improvement because the improved pregnancy rate and outcome can be achieved. Specifically, the unilateral hydrosalpinx with unilateral improvement group had the best prognosis and highest pregnancy rate. Further investigation is required to confirm these findings.
Acknowledgements
The authors would like to thank Guiyuan Zhang and Tingwei Chen for assistance in statistical analyses.
Disclosure statement
All authors declare that they have no competing interests.
Additional information
Funding
References
- Aboulghar, M. A., Mansour, R. T. and Serour, G. I., 1998. Controversies in the modern management of hydrosalpinx. Human Reproduction Update, 4 (6), 882–890.
- Ajonuma, L. C., Ng, E. H. Y. and Chan, H. C., 2002. New insights into the mechanisms underlying hydrosalpinx fluid formation and its adverse effect on IVF outcome. Human Reproduction Update, 8 (3), 255–264.
- Audebert, A. and Pouly, J.L., 2014. Laparoscopic surgery for distal tubal occlusions: lessons learned from a historical series of 434 cases. Fertility and Sterility, 102 (3), e74.
- Chu, J., et al., 2015. Salpingostomy in the treatment of hydrosalpinx: a systematic review and meta-analysis. Human Reproduction (Oxford, England), 30 (8), 1882–1895.
- Cohen, A., Almog, B. and Tulandi, T., 2018. Hydrosalpinx sclerotherapy before in vitro fertilization: systematic review and meta-analysis. Journal of Minimally Invasive Gynecology, 25 (4), 600–607.
- Dreyer, K., et al., 2017. Oil-based or water-based contrast for hysterosalpingography in infertile women. The New England Journal of Medicine, 376 (21), 2043–2052.
- Dunson, D.B., Baird, D.D. and Colombo, B., 2004. Increased infertility with age in men and women. Obstetrics & Gynecology, 103 (1), 51–56.
- Gomel, V., 2015. The place of reconstructive tubal surgery in the era of assisted reproductive techniques. Reproductive Biomedicine Online, 31 (6), 722–731.
- Gomel, V. and Wang, I., 1994. Laparoscopic surgery for infertility therapy. Current Opinion in Obstetrics & Gynecology, 6 (2), 141–148.
- Harb, H.M., et al., 2019. Hydrosalpinx and pregnancy loss: a systematic review and meta-analysis. Reproductive Biomedicine Online, 38 (3), 427–441.
- Hong, X., et al., 2018. Effect of interventional embolization treatment for hydrosalpinx on the outcome of in vitro fertilization and embryo transfer. Medicine, 97 (48), e13143.
- Jansen, R.P.S., 1980. Surgery-pregnancy time intervals after salpingolysis, unilateral salpingostomy, and bilateral salpingostomy. Fertility and Sterility, 34 (3), 222–225.
- Johnson, J.V., Montoya, I.A. and Olive, D.L., 1992. Ethiodol oil contrast medium inhibits macrophage phagocytosis and adherence by altering membrane electronegativity and microviscosity. Fertility and Sterility, 58 (3), 511–517.
- Juneau, C. and Bates, G.W., 2012. Reproductive outcomes after medical and surgical management of ectopic pregnancy. Clinical Obstetrics and Gynecology, 55 (2), 455–460.
- Katler, Q., Pflugner, L. and Martinez, A., 2018. Management of bilateral ectopic pregnancies after ovulation induction using unilateral salpingectomy and methotrexate for the remaining ectopic with subsequent intrauterine pregnancy. Case Reports in Obstetrics and Gynecology, 2018, 7539713–7539714.
- Mage, G., et al., 1986. A preoperative classification to predict the intrauterine and ectopic pregnancy rates after distal tubal microsurgery. Fertility and Sterility, 46 (5), 807–810.
- Ng, K.Y.B. and Cheong, Y., 2019. Hydrosalpinx – Salpingostomy, salpingectomy or tubal occlusion. Best Practice & Research. Clinical Obstetrics & Gynaecology, 59, 41–47.
- Park, S.T., et al., 2017. Clinical characteristics of genital chlamydia infection in pelvic inflammatory disease. BMC Women’s Health, 17 (1), 5.
- Radoń-Pokracka, M., et al., 2019. Evaluation of pregnancy outcomes at advanced maternal age. Open Access Macedonian Journal of Medical Sciences, 7 (12), 1951–1956.
- Simpson, W.L., Beitia, L.G. and Mester, J., 2006. Hysterosalpingography: A Reemerging Study. Radiographics: A Review Publication of the Radiological Society of North America, Inc, 26 (2), 419–431.
- Singhal, V., Li, T. C. and Cooke, I. D., 1991. An analysis of factors influencing the outcome of 232 consecutive tubal microsurgery cases. BJOG: An International Journal of Obstetrics and Gynaecology, 98 (7), 628–636.
- Strandell, A., 2000. The influence of hydrosalpinx on IVF and embryo transfer: a review. Human Reproduction Update, 6 (4), 387–395.
- Strandell, A. and Lindhard, A., 2002. Why does hydrosalpinx reduce fertility?: The importance of hydrosalpinx fluid. Human Reproduction (Oxford, England), 17 (5), 1141–1145.
- Strandell, A., et al., 2001. Hydrosalpinx and IVF outcome: cumulative results after salpingectomy in a randomized controlled trial. Human Reproduction (Oxford, England), 16 (11), 2403–2410.
- Wang, Y., et al., 2011. The impact of advanced maternal age and parity on obstetric and perinatal outcomes in singleton gestations. Archives of Gynecology and Obstetrics, 284 (1), 31–37.
- Xu, B., et al., 2017. Pregnancy outcome of in vitro fertilization after Essure and laparoscopic management of hydrosalpinx: a systematic review and meta-analysis. Fertility and Sterility, 108 (1), 84–95.e5.
- Yohannes, E., et al., 2019. The human tubal lavage proteome reveals biological processes that may govern the pathology of hydrosalpinx. Scientific Reports, 9 (1), 8980.