

Abstract
Female pelvic organ prolapse (POP) is a common condition, which has a high recurrence rate after reconstructive surgery, and the risk factors for POP recurrence are unclear. The aim of this study was to perform a meta-analysis to determine risk factors for POP recurrence. A thorough search of PubMed, Medline, EMBASE, Cochrane Central Register of Controlled Trials, and China Academic Journal Network Publishing Database was conducted for relevant publications until 29 October 2022, without language restrictions. A total of 29 studies involving 6597 patients were included, and the recurrence rate of POP after surgery was 37.7%. Significant OR and CI were found for levator avulsion (OR: 2.46, 95% CI: 1.80–3.36), preoperative stage ≥ III (OR: 1.87, 95% CI: 1.53–2.27), hiatal area on Valsalva manoeuvre (OR: 1.08, 95% CI: 1.03–1.12) and previous pelvic floor surgery (OR: 1.60, 95% CI: 1.07–2.39). Levator avulsion, preoperative stage ≥ III, hiatal area on Valsalva manoeuvre and previous pelvic floor surgery are significant risk factors for POP recurrence.
What is already known on this subject? It has been reported that genetic factors, parity, obesity, birth-induced injury during delivery, etc. are risk factors for POP development and recurrence after operation.
What do the results of this study add? There are few literatures about the risk factors of POP recurrence at present. Our research has increased the information regarding risk factors for POP recurrence.
What are the implications of these findings for clinical practice and/or further research? Our study provides an overview of the risk factors affecting POP recurrence and their contribution (OR, CI) to POP recurrence, which provides valuable evidence-based basis for clinical decision-making in POP treatment and prevention of POP recurrence.
IMPACT STATEMENT
Introduction
Female pelvic organ prolapse (POP) is a common condition in which the weakness of pelvic floor supporting tissue caused by various factors leads to the descending and displacement of pelvic organs and results in the abnormal functions of pelvic organs (Dietz Citation2008). The main symptoms of POP are prolapse of vulvar mass with or without abnormal urination and defaecation, bleeding and inflammation of vulva, etc. POP is common in middle-aged and elderly women, which seriously affects the health and quality of life of those women with symptomatic disorders, and easily induces anxiety, depression, and other mental disorders (Whiteside et al. Citation2004, Delancey et al. Citation2008, Dietz Citation2008). With the increasing ageing of population, POP has attracted more and more attention (Whiteside et al. Citation2004, Delancey et al. Citation2008, Dietz Citation2008, Fritel et al. Citation2009, Friedman, Eslick and Dietz Citation2018). At present, surgery is the main treatment for POP, but it is well known that the reoperation rate of reconstructive surgery is very high. According to the literature, the recurrence rate of POP after reconstructive surgery can be as high as 58% (Whiteside et al. Citation2004, Delancey et al. Citation2008, Fritel et al. Citation2009, Friedman et al. Citation2018). To date, little is known about the risk factors associated with recurrence after reconstructive surgery. It is therefore very important to identify risk factors for POP recurrence to provide proper preoperative counselling or tailor most appropriate surgical treatment approaches. In recent years, it has been reported that genetic factors, parity, obesity, birth-induced injury during delivery, etc. are risk factors for POP development and recurrence after operation (Tegerstedt and Hammarström Citation2004, Diez-Itza, Aizpitarte and Becerro Citation2007, Delancey et al. Citation2008, Fritel et al. Citation2009, Friedman et al. Citation2018). However, it’s difficult to weigh the importance of risk factors for POP recurrence reported in the literatures. The purpose of our study was to perform a meta-analysis to determine risk factors for recurrence after reconstructive operation for POP.
Materials and methods
A thorough search of PubMed, Medline, EMBASE, Cochrane Central Register of Controlled Trials, China Academic Journal Network Publishing Database was conducted for relevant publications until 29 October 2022. The search strategy was performed with the following search terms both medical subject headings (MeSH) terms and free-text terms including Pelvic Organ Prolapse or Urogenital prolapse or Genital prolapse or Cystocele or Bladder Prolapse and Relapse or Recurrence or Reoperation and Risk factors or Predictors. The searched literature was managed and screened by the document management software Endnote X8. There were no language restrictions, and ethical approval was not required.
At first, the titles and abstracts of all the obtained studies were evaluated by two investigators to identify potentially relevant articles. Then, they reviewed independently the full texts of potentially relevant articles for inclusion. Any disagreements between the two observers were resolved by discussing with one of the other researchers in the research group until a consensus was obtained.
After the final selection, the data extraction was performed using a standardised data extraction form with information including authors, publication year, study design and conduct, study population type, total sample size, mean age, data on risk factors investigated for recurrence of POP or risk estimate reported as odds ratio (OR) or data used to calculate OR, and 95% confidence interval (CIs) or data used to calculate CIs.
Statistical analysis
Meta-analyses were conducted using the statistical tool Stata 15 software. ORs and 95% CIs were calculated for the effects on the risk of female POP recurrence. Assessment of heterogeneity was performed in accordance with the guidance in the Cochrane Handbook for Systematic Reviews of Interventions (Higgins and Green Citation2011). Heterogeneity was tested using with Cochran’s Q test, with p < 0.05 indicating heterogeneity, and the degree of heterogeneity was quantified using the I2 test, which represents the percentage of total heterogeneity variability across studies, with an I2 statistic greater than 50% indicating statistically heterogeneity. When I2 is more than 50% and Q test p < 0.05, suggesting that there is obvious heterogeneity among the studies, the random effects model was used. If I2 is less than 50%, and Q test p > 0.05, suggesting that there is no significant heterogeneity, and the fixed effects model was applied for pooling of data. Egger’s and Begg’s test, which are the most common statistical tests used for detecting asymmetric funnel plot, were performed to investigate the publication bias (Sterne et al. Citation2009, van Enst et al. Citation2014).
Results
Description of included studies
A total of 2637 articles were evaluated at the initial search. After careful examination of the titles, abstracts, or full texts, 29 studies were finally included. shows the flow diagram of the selection process. The characteristics of these studies are summarised in . These studies, including cohort studies and case-control studies, were conducted in Europe, America, Australia and Asia, respectively. A total of 6597 patients were included. Of these, 2419 cases had recurrence after operation for POP, with a recurrence rate of 37.7%.
Figure 1. Flow diagram of the selection process.
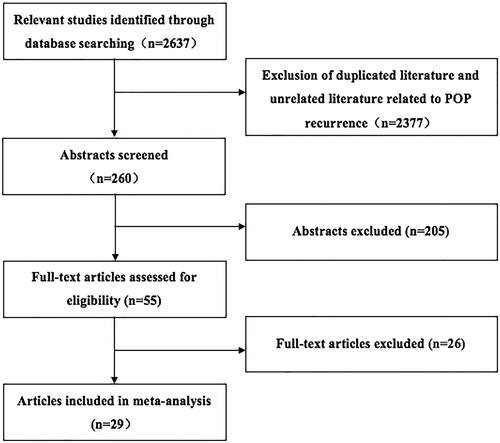
Table 1. Characteristics of included studies.
Risk factors for POP recurrence
Because there are many parameter associated with POP recurrence in identified papers, meta-analysis was carried out only for those related factors reported in three or more literatures in this study, including levator avulsion, previous pelvic floor surgery, preoperative stage ≥ III-IV, history of hysterectomy, smoker, overweight or obese, parity, menopause, chronic pulmonary diseases, constipation, diabetes and hiatal area on Valsalva manoeuvre. The relationship between risk factors and POP recurrence after surgery is shown in . From , it can be seen that the risk factors for recurrence of POP are associated with levator avulsion (OR: 2.46, 95% CI: 1.80–3.36, ), preoperative stage ≥ III (OR: 1.87, 95% CI: 1.53–2.27, ), hiatal area on Valsalva manoeuvre (OR: 1.08, 95% CI: 1.03–1.12, Figure S1) and previous pelvic floor surgery (OR: 1.60, 95% CI: 1.07–2.39, Figure S2). However, there was not statistically significant for the effects of overweight or obesity, parity, menopause, smoker, history of hysterectomy, constipation, chronic pulmonary diseases, diabetes mellitus on POP recurrence after surgery (Figure S3–S10).
Figure 2. Meta-analysis of association between levator avulsion and pelvic organ prolapse (POP) recurrence. Each study is shown by an odds ratio estimate with the corresponding 95% confidence interval.
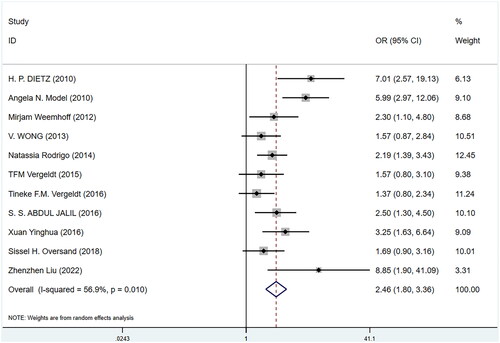
Figure 3. Meta-analysis of association between preoperative stage(III-IV)and pelvic organ prolapse (POP) recurrence. Each study is shown by an odds ratio estimate with the corresponding 95% confidence interval.
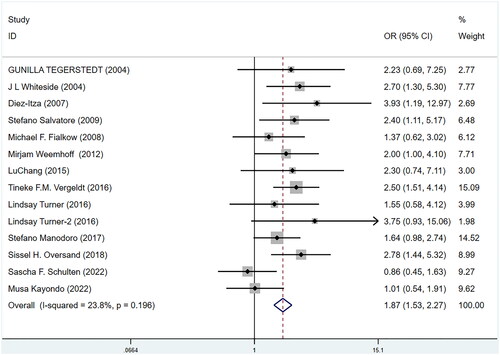
Table 2. The meta-analysis of risk factors for the recurrence of POP after surgery.
Sensitivity analysis and publication bias
In the sensitivity analyses, the pooled odds ratios (OR) of all risk factors assessed were calculated by both fixed and random effect models. Except for the risk factor of parity, the other assessed factors yielded similar results, indicating the reliability and stability of the pooled results. Moreover, except for the risk factor of levator avulsion, there was no evidence of publication bias based on Egger’s and Begg’s regression analysis for the rest of the any of the risk factors assessed ().
Table 3. Sensitivity analysis and publication bias.
Discussion
This meta-analysis evaluated 29 studies published up to October 2022, in which 6597 women with POP following surgical treatment were studied for risk factors of recurrence. Our study provides an overview of the risk factors affecting POP recurrence and their contribution (OR, CI) to POP recurrence. The following risk factors were investigated including levator avulsion, previous pelvic floor surgery, preoperative stage ≥ III-IV, history of hysterectomy, smoker, overweight or obese, parity, menopause, chronic pulmonary diseases, constipation, diabetes and hiatal area on Valsalva manoeuvre in our study. Although these risk factors have been analysed by other studies (Tegerstedt and Hammarström Citation2004, Diez-Itza et al. Citation2007, Fialkow et al. Citation2008, Fritel et al. Citation2009, Friedman et al. Citation2018), our analysis shows these factors does not always have statistical significance. Regarding POP recurrence, we found that only levator avulsion, preoperative stage ≥ III, hiatal area on Valsalva manoeuvre and previous pelvic floor surgery were the most important risk factors. There are few studies about the risk factors of POP recurrence at present. Our research has increased the information regarding risk factors for POP recurrence, which provides a valuable evidence-based basis for clinical decision-making in POP treatment and prevention of POP recurrence.
With the ageing of population, POP has gradually become a common disease which does harm to the health of women with symptomatic disorders. The aetiology of POP is still unknown. Many factors that women encounter in their lifetime, such as abnormal anatomy, genetic factors, living habits, production injuries and complications, seem to be involved in the occurrence and development of POP(Fritel et al. Citation2009, Friedman et al. Citation2018, Tegerstedt and Hammarström Citation2004). Surgery including total hysterectomy, anterior vaginal wall repair and posterior vaginal wall repair and so on is still the most effective treatment for POP. However, surgery for POP is known to have a high recurrence rate of 36% (Tegerstedt and Hammarström Citation2004, Diez-Itza et al. Citation2007, Fialkow et al. Citation2008, Friedman et al. Citation2018). In our meta-analysis evaluated 29 studies, we found that recurrence rate of POP after surgery was 37.7%. This result is in agreement with previous findings from Friedman et al. (Citation2018). Therefore, it is very important to find out the risk factors of POP recurrence and actively prevent recurrence of POP. It is known that maintaining the normal position of female genital organs depends on normal anatomical structure and function of the pelvic floor muscles, fascia and uterine ligaments (Tegerstedt and Hammarström Citation2004, Diez-Itza et al. Citation2007, Fialkow et al. Citation2008, Denman et al. Citation2008, Friedman et al. Citation2018). Pelvic floor tissue degeneration, trauma, congenital dysplasia or damage caused by some diseases result in reduced tension and weakened support function, and further cause female reproductive organs and adjacent organs to move down, finally leading to POP. A series of studies have shown that risk factors for POP include age, BMI, parity, family history of POP, levator avulsion, diabetes mellitus and other chronic diseases (Tegerstedt and Hammarström Citation2004, Diez-Itza et al. Citation2007, Fialkow et al. Citation2008, Denman et al. Citation2008, Salvatore et al. Citation2009, Vergeldt et al. Citation2015). Some risk factors above-mentioned may also be the risk factors of POP recurrence, such as parity, family history of POP, levator avulsion, etc. Therefore, it is helpful to identify risk factors for POP recurrence to guide the choice of treatment and operation for POP patients, and to provide guidance for clinical prevention of POP recurrence. In agreement with previous studies (Abdul Jalil et al. Citation2016, Rappa and Saccone Citation2016, Turner et al. Citation2016, Cho, Moon and Kim Citation2017), we have shown that levator avulsion, preoperative stage ≥ III, hiatal area on Valsalva manoeuvre and previous pelvic surgery history are risk factors for POP recurrence, and overweight or obesity, parity, menopause, smoker, history of hysterectomy, constipation, chronic pulmonary diseases, diabetes mellitus are not associated with POP recurrence.
Meta-analysis is carried out based on summarising the previous research literature. While enlarging the sample size and improving the credibility of the conclusions, it may also accumulate the bias of the corresponding original literature. Therefore, there are several limitations of our study: First, because there are the differences in definitions of recurrent prolapse and the inclusion criteria of each study, as well as the huge differences in definitions of risk factors, our ability to compare and use all available information in statistical analysis has been narrowed in our meta-analysis. Second, some literature included in this meta-analysis has low qualities, for example, some studies reported incomplete information or no extractable data which made meta-analysis were unavailable, resulting in the loss of information. Third, there is publication bias detected in the risk factor of levator avulsion which may come from the process of searching for literature published in English and Chinese. Finally, data were obtained largely from retrospective studies, and some of which have similar population size, which is an additional limitation of this study. Despite these limitations, the strength of this study was that we used appropriate statistical methods to generate pooled estimates and explored possible the heterogeneity. In addition, our research is systematic and comprehensive review including the large population size (29 studies published over 18 years from the whole world, and more than 6,000 patients).
In conclusion, our meta-analysis demonstrated that preoperative POP score (> III), hiatal area on Valsalva manoeuvre, pelvic surgery history and levator avulsion were risk factors for POP recurrence. Therefore, in order to reduce clinically the POP recurrence rate after operation, patients with the risk factors identified in this meta-analysis should be given more detailed preoperative consultation, more cautious tailoring most appropriate treatment approaches: conservative or surgical, and postoperative care and patient education should be strengthened.
Supplemental Material
Download Zip (2.6 MB)Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Abdul Jalil, S.S., Guzman Rojas, R. and Dietz, H.P., 2016. Does it matter whether levator avulsion is diagnosed pre- or postoperatively? Ultrasound in Obstetrics & Gynecology, 48 (4), 516–519.
- Bodner-Adler, B., et al., 2022. Clinical risk factors for recurrence of pelvic organ prolapse after primary native tissue prolapse repair. Wiener Klinische Wochenschrift, 134 (1–2), 73–75.
- Cho, M.K., Moon, J.H. and Kim, C.H., 2017. Factors associated with recurrence after colpocleisis for pelvic organ prolapse in elderly women. International Journal of Surgery, 44, 274–277.
- Delancey, J.O., et al., 2008. Graphic integration of causal factors of pelvic floor disorders: an integrated life span model. American Journal of Obstetrics and Gynecology, 199 (6), 610.e1–610–e6105.
- Denman, M.A., et al., 2008. Reoperation 10 years after surgically managed pelvic organ prolapse and urinary incontinence. American Journal of Obstetrics and Gynecology, 198 (5), 555.e1–555.e5555–555.e5.
- Dietz, H.P., Chantarasorn, V. and Shek, K.L., 2010. Levator avulsion is a risk factor for cystocele recurrence. Ultrasound in Obstetrics & Gynecology, 36 (1), 76–80.
- Dietz, H.P., 2008. The aetiology of prolapse. International Urogynecology Journal, 19 (10), 1323–1329.
- Diez-Itza, I., Aizpitarte, I. and Becerro, A., 2007. Risk factors for the recurrence of pelvic organ prolapse after vaginal surgery: a review at 5 years after surgery. International Urogynecology Journal and Pelvic Floor Dysfunction, 18 (11), 1317–1324.
- Edenfield, A.L., et al., 2013. Vaginal prolapse recurrence after uterosacral ligament suspension in normal-weight compared with overweight and obese women. Obstetrics and Gynecology, 121 (3), 554–559.
- Fialkow, M.F., Newton, K.M. and Weiss, N.S., 2008. Incidence of recurrent pelvic organ prolapse 10 years following primary surgical management: a retrospective cohort study. International Urogynecology Journal and Pelvic Floor Dysfunction, 19 (11), 1483–1487.
- Friedman, T., Eslick, G.D. and Dietz, H.P., 2018. Risk factors for prolapse recurrence: systematic review and meta-analysis. International Urogynecology Journal, 29 (1), 13–21.
- Fritel, X., et al., 2009. Symptomatic pelvic organ prolapse at midlife, quality of life, and risk factors. Obstetrics and Gynecology, 113 (3), 609–616.
- Higgins, J., Green, S.R., 2011. Cochrane handbook for systematic review of interventions Version 5.1.0 (updated March 2011). The Cochrane Collaboration. Training.cochrane.org/handbook/archive/v5.1/
- Jin, L., Wang, J. and Zhang, X., 2005. Clinical analysis of the relapse and its related factors in patients with pelvic organ prolapse. Chinese Journal of Clinical Obstetric and Gynecology, 6 (1), 8–12.
- Kayondo, M., et al., 2022. Risk factors for recurrence of pelvic organ prolapse after vaginal surgery among Ugandan women: a prospective cohort study. International Urogynecology Journal, 33 (7), 1933–1939.
- Kim, J.H., et al., 2022. Outcomes of vaginal hysterectomy combined with anterior and posterior colporrhaphy for pelvic organ prolapse: a single center retrospective study. Obstetrics & Gynecology Science, 65 (1), 74–83.
- Liu, Z., et al., 2022. Clinical and pelvic floor ultrasound characteristics of pelvic organ prolapse recurrence after transvaginal mesh pelvic reconstruction. BMC Women’s Health, 22 (1), 102.
- Lu, C., Wei, W. and Lu, D., 2015. The risk factors for pelvic organ prolapse treated by traditional surgical procedures. Chinese Clinical Doctor, 43, 76–79.
- Manodoro, S., et al., 2018. Risk factors for recurrence after hysterectomy plus native-tissue repair as primary treatment for genital prolapse. International Urogynecology Journal, 29 (1), 145–151.
- Model, A.N., Shek, K.L. and Dietz, H.P., 2010. Levator defects are associated with prolapse after pelvic floor surgery. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 153 (2), 220–223.
- Oversand, S.H., et al., 2019. Impact of levator muscle avulsions on Manchester procedure outcomes in pelvic organ prolapse surgery. Acta Obstetricia et Gynecologica Scandinavica, 98 (8), 1046–1054.
- Rappa, C. and Saccone, G., 2016. Recurrence of vaginal prolapse after total vaginal hysterectomy with concurrent vaginal uterosacral ligament suspension: comparison between normal-weight and overweight women. American Journal of Obstetrics and Gynecology, 215 (5), 601.e1–601–e4.
- Rodrigo, N., et al., 2014. The use of 3-dimensional ultrasound of the pelvic floor to predict recurrence risk after pelvic reconstructive surgery. The Australian & New Zealand Journal of Obstetrics & Gynaecology, 54 (3), 206–211.
- Salvatore, S., et al., 2009. Identification of risk factors for genital prolapse recurrence. Neurourology and Urodynamics, 28 (4), 301–304.
- Schulten, S.F., et al., 2022. Risk factors for pelvic organ prolapse recurrence after sacrospinous hysteropexy or vaginal hysterectomy with uterosacral ligament suspension. American Journal of Obstetrics and Gynecology, 227 (2), 252.e1–252–e9.
- Sterne, J.A., Egger, M. and Moher, D., 2009. Adressing reporting bias; detecting repoting bias. In: J.P.T. Higgins, S. Green, eds. Oxford: Wiley-Blackwell. 310–324.
- Tegerstedt, G. and Hammarström, M., 2004. Operation for pelvic organ prolapse: a follow-up study. Acta Obstetricia et Gynecologica Scandinavica, 83 (8), 758–763.
- Turner, L., et al., 2016. The impact of obesity on intraoperative complications and prolapse recurrence after minimally invasive sacrocolpopexy. Female Pelvic Medicine & Reconstructive Surgery, 22 (5), 317–323.
- van Enst, W.A., et al., 2014. Investigation of publication bias in meta-analyses of diagnostic test accuracy: a meta-epidemiological study. BMC Medical Research Methodology, 14, 70.
- Vergeldt, T.F., et al., 2015. Levator hiatal area as a risk factor for cystocele recurrence after surgery: a prospective study. BJOG : An International Journal of Obstetrics and Gynaecology, 122 (8), 1130–1137.
- Vergeldt, T.F., et al., 2016. Anatomical Cystocele Recurrence: Development and Internal Validation of a Prediction Model. Obstetrics and Gynecology, 127 (2), 341–347.
- Weemhoff, M., et al., 2012. Avulsion of puborectalis muscle and other risk factors for cystocele recurrence: a 2-year follow-up study. International Urogynecology Journal, 23 (1), 65–71.
- Whiteside, J.L., et al., 2004. Risk factors for prolapse recurrence after vaginal repair. American Journal of Obstetrics and Gynecology, 191 (5), 1533–1538.
- Wong, V., et al., 2013. Is levator avulsion a predictor of cystocele recurrence following anterior vaginal mesh placement? Ultrasound in Obstetrics & Gynecology : The Official Journal of the International Society of Ultrasound in Obstetrics and Gynecology, 42 (2), 230–234.
- Xuan, Y., et al., 2016. Study on postoperative application of trasnspreineal 3d ultrasound for pelvic organ prolapse. Chinese Journal of Clinical Obstetrics and Gynecology, 17 (3), 216–219.
- Yang, J., et al., 2022. Long-term observation on postoperative recurrence and complications of transvaginal mesh surgery for pelvic organ prolapse. Gynecologic and Obstetric Investigation, 87 (1), 30–37.