

 ?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.
?Mathematical formulae have been encoded as MathML and are displayed in this HTML version using MathJax in order to improve their display. Uncheck the box to turn MathJax off. This feature requires Javascript. Click on a formula to zoom.Abstract
Pregnant women are one of the endangered groups who need special attention in the COVID-19 epidemic. We conducted a systematic review and summarised the studies that reported adverse pregnancy outcomes in pregnant women with COVID-19 infection. A literature search was performed in PubMed and Scopus up to 1 September 2022, for retrieving original articles published in the English language assessing the association between COVID-19 infection and adverse pregnancy outcomes. Finally, in this review study, of 1790 articles obtained in the initial search, 141 eligible studies including 1,843,278 pregnant women were reviewed. We also performed a meta-analysis of a total of 74 cohort and case-control studies. In this meta-analysis, both fixed and random effect models were used. Publication bias was also assessed by Egger’s test and the trim and fill method was conducted in case of a significant result, to adjust the bias. The result of the meta-analysis showed that the pooled prevalence of preterm delivery, maternal mortality, NICU admission and neonatal death in the group with COVID-19 infection was significantly more than those without COVID-19 infection (p<.01). A meta-regression was conducted using the income level of countries. COVID-19 infection during pregnancy may cause adverse pregnancy outcomes including of preterm delivery, maternal mortality, NICU admission and neonatal death. Pregnancy loss and SARS-CoV2 positive neonates in Lower middle income are higher than in High income. Vertical transmission from mother to foetus may occur, but its immediate and long-term effects on the newborn are unclear.
Introduction
Severe acute respiratory syndrome caused by COVID-19 (SARS-CoV-2) is an emerging and rapidly evolving situation and a global public health emergency and crisis that can cause severe lung disease and death (World Health Organization Citation2020). The spread of this virus has caused a devastating epidemic, challenged health and social services and led to high mortality rates that vary according to the epidemiological and social characteristics of each country (Mascarenhas et al. Citation2020). Despite efforts to control the pathogen, COVID-19 was considered a pandemic by the WHO on 11 March 2020 (Silva et al. Citation2020).
Clinical manifestations of this disease range from asymptomatic cases and mild upper airway infection to severe and fatal cases with pneumonia and acute respiratory failure (Lopes de Sousa et al. Citation2020). Studies to date have shown that the clinical, radiological and laboratory features of COVID-19 pneumonia in pregnant women are similar to those reported in non-pregnant patients (Chen et al. Citation2020, Yu et al. Citation2020).
Pregnant women are a high-risk population for infectious respiratory diseases. This may be due to physiological and anatomical changes, such as an increase in the transverse diameter of the chest, diaphragm elevation, decreased lung capacity and functional residual volumes, increased heart rate and oxygen consumption, respiratory tract mucosa oedema, and increased secretions in the upper respiratory tract following vasodilation (O'Day Citation1997, Ramsey and Ramin Citation2001, Mosby et al. Citation2011, Mertz et al. Citation2013, Chen et al. Citation2020, Liu et al. Citation2020a, Citation2020c). These alterations may increase the risk of more severe disease compared with no pregnant adults. In addition to these mechanical changes, immunological adaptation is essential to ensure maternal tolerance to the foetus, which makes pregnant women a more vulnerable group (Silva et al. Citation2020). The first and third trimesters of pregnancy can be considered periods of increased inflammatory activity, while the second trimester is a period of decreased overall immune system activity (Mor et al. Citation2017, Liu et al. Citation2020b). Changes in cell-mediated immunity lead to increased susceptibility of pregnant women to being infected with intracellular organisms such as viruses (Zaigham and Andersson Citation2020).
Considering the importance of pregnancy outcomes, it is essential to obtain knowledge about pregnancy outcomes during the COVID-19 epidemic, including the severity of symptoms in pregnant women, possible complications during pregnancy, the possibility of vertical transmission, and the condition of infected infants.
In this way, healthcare workers can be adequately equipped with knowledge about the prognoses and management of pregnant women with COVID-19. Although studies on pregnancy outcomes in COVID-19 are increasing, most of them are case reports or case series with small population samples and conflicting results and the majority of cohort studies have focussed on evaluating the effects of COVID-19 on the general population. Additionally, there is a wide variation in the methodology and data reporting in recently published articles, making accurate data interpretation difficult.
The aim of this study was to conduct a systematic review and meta-analysis of the published literature on pregnancy with COVID-19 to evaluate the effect of this novel infection on maternal, perinatal and neonatal outcomes.
Methods
The present systematic review was conducted based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) (Moher et al. Citation2009). This study was approved by the Research Ethics Committees of Vice-Chancellor in Research Affairs-Shahid Beheshti University of Medical Sciences (approval code: IR.SBMU.RETECH.REC.1399.760); and the study was registered in the International Prospective Register of Systematic Reviews (PROSPERO) (code: CRD42022360777). The PICO question of this study was: in pregnant women with COVID-19 infection, what are adverse pregnancy outcomes, compared to those without COVID-19?
Search strategy
An electronic literature search was conducted independently by two authors, who were familiar with search methods and information sources, without any restrictions, in the PubMed (including Medline) and Scopus databases for retrieving original articles published in English language assessing the association between COVID-19 infection and adverse pregnancy outcomes up to 1 September 2022. Furthermore, to maximise the identification of eligible studies, reference lists of relevant articles and reviews included were manually evaluated as well. The following keywords, either alone or in combination, were used for the search: (‘coronavirus’ OR ‘COVID-19’ OR ‘SARS-CoV-2’ OR ‘SARS-2’ OR ‘2019-nCoV’ OR ‘2019 novel coronavirus’) AND (‘pregnancy’ OR ‘pregnant women’ OR ‘maternal’ OR ‘gestational’) AND (‘adverse pregnancy outcomes’ OR ‘pregnancy outcomes’ OR ‘pregnancy complications’ OR ‘neonatal outcomes’ OR ‘abortion’ OR ‘miscarriage’ OR ‘pregnancy loss’ OR ‘fetal death’ OR ‘stillbirth’ OR ‘preeclampsia’ OR ‘gestational hypertension’ OR ‘pregnancy-induced hypertension’ OR ‘PIH’ OR ‘gestational diabetes’ OR ‘GDM’ OR ‘hemorrhage’ OR ‘postpartum hemorrhage’ OR ‘PPH’ OR ‘Placenta abruption’ OR ‘placenta previa’ OR ‘preterm’ OR ‘premature rupture of membrane’ OR ‘PROM’ OR ‘Intrauterine growth restriction’ OR ‘IUGR’ OR ‘small for gestational age’ OR ‘SGA’ OR ‘Low birth weight’ OR ‘LBW’ OR ‘oligohydramnios’ OR ‘Apgar’ OR ‘fetal distress’ OR ‘SARS-CoV-2 infection of the neonate’ OR ‘neonatal distress’ OR ‘RDS’ OR ‘neonatal death’ OR ‘neonatal mortality’ OR ‘neonatal admission’ OR ‘NICU admission’ OR ‘malformation’ OR ‘anomalies’). Table S1 shows search strategy of the study.
Selection criteria, study selection and data extraction
In this systematic review and meta-analysis, all the studies with an observational design including case-series, cross-sectional, case-control, and prospective or retrospective cohort studies were included.
Studies were included if they met the following criteria: (1) the study population included pregnant women who had COVID-19 infection confirmed by positive viral SARS-CoV-2 RNA testing; (2) the outcome of interest was at least one adverse pregnancy outcome.
We also excluded non-original studies including guidelines, review articles, case reports, animal studies, studies performed in vitro, commentaries, editorials, correspondences, letters to the editor, meeting abstracts, as well as studies that did not provide accurate and clear data.
After removing duplicates recognised in databases and reference lists, titles and abstracts were screened to evaluate the suitability of the manuscript based on the final eligibility criteria.
The first assessment, carried out by three investigators (SN, MS and ASh). Disagreements were resolved through scientific discussions. The general characteristics of the studies, including the first author’s name, article title, journal name, country of study, publication year, study design, sample size, population characteristics and pregnancy outcomes were extracted from the studies and assessed. To prevent extraction and data entry errors, a control check between the final data used in the systematic review and the original publications was conducted by all authors.
Quality assessment
All studies included in the present systematic review were critically appraised for the quality of their methodological and the presented results. Three reviewers, blinded to study author, journal name and institution, evaluated the quality of the studies independently using the Critical Appraisal Checklist recommended by the Joanna Briggs Institute for a variety of studies (cohort, case-control, cross-sectional and case series studies) (Munn et al. Citation2019), and disagreements were resolved by consensus. The Joanna Briggs Institute Critical Appraisal tools included eight questions for cross-sectional and case series studies, nine questions for reporting prevalence data, 10 questions for case-control studies and 11 questions for cohort studies, that reviewers addressed for each study. The answer ‘yes’ to each question received one point. Thus, the final scores for each study could range from 0 to 8, 0 to 9, 0 to 10 and 0 to 11 for cross-sectional and case series studies, reporting prevalence data, case-control studies and cohort studies, respectively. Table S2 shows results of quality assessment of included studies.
Outcome measures in meta-analysis
Maternal, neonatal and foetal outcomes of interest were categorised into 10 outcomes, including five composite outcomes including: (1) preterm delivery was defined as birth below 37 weeks of gestation (preterm <34 weeks, and <37 weeks), (2) pregnancy loss was defined as death of an unborn baby (foetus) at any time during pregnancy (abortion, foetal death, foetal loss, still birth), (3) PROM was defined as rupture (breaking open) of the membranes (amniotic sac) before labour begins (PROM and PPROM), (4) IUGR/SGA was described a foetus that has not reached its growth potential (IUGR) and/or an infant whose birth weight was below the 10th percentile for the appropriate gestational age (SGA), (5) hypertension disorders of pregnancy (PIH, preeclampsia and severe preeclampsia, eclampsia), (6) GDM was defined as any degree of glucose intolerance with onset or first recognition during pregnancy, (7) maternal mortality was defined as the death of a woman from direct or indirect obstetric causes, (8) LBW defined an infant born weighing 2500 g or less, (9) NICU admission was defined as the admission of a Neonatal Intensive Care Unit and (10) neonatal death was defined as the death of a live born infant, regardless of gestational age at birth, within the first 28 completed days of life.
Statistical analysis
This study was conducted to estimate the pooled prevalence of pregnancy adverse outcomes in COVID-19 infected mothers. In addition, we compared the prevalence of outcomes with the control groups in case of data availability. The ‘Meta-prop’ using the Mantel–Haenszel method was applied to estimate the prevalence of outcomes in each group. The heterogeneity was assessed using I-squared statistics considering the threshold of 50% and the p value less than .05 for the significance of the related test. In this regard, we selected the random effect model if the data heterogeneity was confirmed. For the other situations, the fixed effect model was chosen. The difference between subgroups was explored using Chi-squared statistics at the significant level of .05.
We explored the publication bias using the graphical approach funnel plot and Egger’s test. In case of a p value less than .05 for the Egger test, we applied the trim and filled method. The forest plots for all outcomes pooled prevalence were depicted. All these plots included the study-specific data and the random and fixed effect pooled prevalence.
A meta-regression approach was used to explore the impact of geographical and economic variations on the outcomes. In this manner, the prevalence regresses on the income level of countries. The countries were classified as high income, lower middle income or upper middle income using income level of countries according to the World Bank classification (Bank Citation2021).
All the analysis and graphical presentations were done in R statistical software version 4.0.5 (R Foundation for Statistical Computing, Vienna, Austria) and the ‘meta’ library in this environment. All the confidence intervals were reported at 95%, and the tests were considered significant if the p value was calculated as less than .05.
Results
Search results and study selection
As the flowchart of the literature search in shows, the search strategy yielded 1790 potentially relevant articles. Based on selection inclusion criteria, 213 articles were identified for further full-text assessment. We included 141 studies, which included data from 1,843,278 pregnant women for this systematic review.
Figure 1. Flowchart of the literature search for the systematic review.
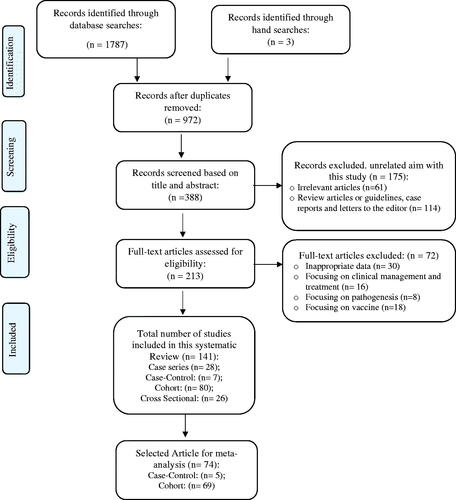
Out of 141 studies included, seven were case-control, 28 were case series, 26 were cross-sectional and 80 were cohort studies. Finally, a total of 74 including 69 cohort and five case-control studies were included in this meta-analysis. shows the characteristics of cohort and case-control studies included in the meta-analysis.
Table 1. Characteristics of cohort and case-control studies included in the meta-analysis.
The articles were published in various geographical regions. Most studies were conducted in China (45 studies) or the United States (34 studies). Ten studies compared the pregnancy outcomes before and during the COVID-19 pandemic or lockdown (Ashish et al. Citation2020, Justman et al. Citation2020, Cauldwell et al. Citation2021, Du et al. Citation2021, Goyal et al. Citation2021, Kirchengast and Hartmann Citation2021, Ranjbar et al. Citation2021, Rotshenker-Olshinka et al. Citation2021, Shakespeare et al. Citation2021, Wilk et al. Citation2021). Tables S3–S6 show the summary of the main characteristics of the studies included in the systematic review.
Meta-analysis of outcomes
Figures S1–S11 illustrate the forest plots of the pooled prevalence of pregnancy outcomes in pregnant women with and without Covid infection. Results showed that the pooled prevalence of preterm delivery, maternal mortality, NICU admission and neonatal death in the group with COVID-19 infection (14.32 (95% CI: 12.07, 16.91), 0.65 (95% CI: 90.37, 1.130), 14.57 (95% CI: 10.15, 20.48), 0.65 (95% CI: 0.51, 0.83), respectively) were significantly more than those without COVID-19 infection (5.57 (95% CI: 3.2, 9.52), 0.02 (95% CI: 0.01, 0.11), 4.53 (95% CI: 2.45, 8.22), 0.06 (95% CI: 0.05, 0.08), respectively).
There was no significant difference in the pooled prevalence of other pregnancy outcomes including PROM, GDM, hypertensive disorders, IUGR/SGS, LBW, PPH and pregnancy loss. The pooled prevalence of SARS-CoV2 positive neonates was 2.04 (95% CI: 1.71; 2.45).
The meta-regression results showed that the mean prevalence of pregnancy loss in lower middle income and upper middle-income countries were 1.23% (p value = .03) and 1.27% (p value = .001) higher than in high-income countries, respectively. The mean prevalence of SARS-CoV2 positive neonates in lower middle income was 1.04% higher than in high-income countries (p value = .009). While the mean prevalence of PPH in lower middle-income countries was 1.3% lower than high-income countries (p value = .016). shows results of the meta-regression using income level of countries (according to the World Bank classification).
Table 2. Results of the meta-regression using income level of countries (according to the World Bank classification).
Publication bias
Figures S12–S23 show the funnel plots of the results of publication biases based on Egger’s test in adverse pregnancy outcomes.
Egger’s test shows significant publication biases among studies investigating the prevalence of hypertensive disorders (p value = .02), LBW (p value=.03), maternal mortality (p value < .001) and pregnancy loss (p value < .001) which were adjusted by the trim and fill method. Figures S24–S27 show the results of the trim and fill of these pregnancy outcomes.
Quality assessment
Quality assessment based on the Critical Appraisal Checklist showed that among seven case-control studies, four studies were classified as being of high quality (8–10 score) and three studies had moderate quality (5–7 score); among 28 case series, 18 studies were classified as being of high quality (7–8 score) and 10 studies had moderate quality (5–6 score); among of 26 cross-sectional, two studies were classified as being of high quality (7–8 score), 22 studies had moderate quality (5–6 score) and two studies had low quality (≤4 scores); among 80 cohort studies, 67 studies were classified as being of high quality (9–11 score) and 13 studies had moderate quality (6–8 score). As shown in Table S2, among the total of 141 studies, 71.5% had high quality, 44.2% medium and the rest (two articles) had low quality.
Feto-maternal outcomes
Comparison of outcomes in patients with or without COVID-19 in included analytical studies showed a significant difference in the outcomes of preterm birth (Marín Gabriel et al. Citation2020, Abedzadeh‐Kalahroudi et al. Citation2021, Chinn et al. Citation2021, Cruz Melguizo et al. Citation2021, Gupta et al. Citation2021, Katz et al. Citation2021, Milln et al. Citation2021, Taghavi et al. Citation2021, Timircan et al. Citation2021), PROM (Cruz-Lemini et al. Citation2021, Cruz Melguizo et al. Citation2021, Du et al. Citation2021, Timircan et al. Citation2021), PPROM (Cruz Melguizo et al. Citation2021), prematurity, GDM (Ko et al. Citation2021), gestational hypertension (Ko et al. Citation2021), pre-eclampsia/eclampsia (severe pre-eclampsia and moderate pre-eclampsia) (Abedzadeh‐Kalahroudi et al. Citation2021, Cruz Melguizo et al. Citation2021, Ko et al. Citation2021, Wilk et al. Citation2021), foetal distress (Abedzadeh‐Kalahroudi et al. Citation2021, Gupta et al. Citation2021), stillbirth (Cruz Melguizo et al. Citation2021), pregnancy morbidity (Tadas et al. Citation2021), IUFD (Hcini et al. Citation2021), PPH (Hcini et al. Citation2021), maternal mortality (Chinn et al. Citation2021), and prolonged labour (Wilk et al. Citation2021). Maternal mortality has been reported in 26 studies, but only in one analytical study there was a significant difference between patients with and without COVID-19 infection (Chinn et al. Citation2021).
Some studies have compared the pregnancy outcomes before and during the COVID-19 pandemic. The results of these studies have also been different. Some studies showed a significant difference in pregnancy outcomes such as high-risk pregnancies (Goyal et al. Citation2021), GDM, PROM (Du et al. Citation2021), hypertensive disorders/pre-eclampsia (Justman et al. Citation2020, Wilk et al. Citation2021), stillbirth (Ashish et al. Citation2020), prolonged labour (Wilk et al. Citation2021), between two periods, while other studies reported no significant change in maternal mortality or severe maternal morbidity (such as PPH, uterine rupture and severe preeclampsia/eclampsia) and stillbirth (Shakespeare et al. Citation2021).
Neonatal outcomes
Comparison of outcomes in patients with or without COVID-19 in included analytical studies showed a significant difference in the outcomes of prematurity (Timircan et al. Citation2021), NICU admission (Cruz-Lemini et al. Citation2021, Cruz Melguizo et al. Citation2021), neonatal admission (Milln et al. Citation2021) and birth weight (Gupta et al. Citation2021).
The comparison of neonatal outcomes in the two periods (before and during the COVID-19 pandemic) was not the same. Some studies have reported an increase in neonatal mortality (Du et al. Citation2021, Wilk et al. Citation2021), while some studies showed no significant change in NICU admissions or other outcomes (Justman et al. Citation2020, Du et al. Citation2021, Shakespeare et al. Citation2021, Wilk et al. Citation2021, Wagner et al. Citation2022).
Discussion
Since the onset of the COVID-19 epidemic in early 2020, there has been concern that the disease in pregnant women may have adverse effects on pregnancy outcomes. In this systematic review and meta-analysis, we summarise the result of 141 studies. The clinical characteristics, radiological and laboratory manifestations are similar in pregnant women with COVID-19 infection when compared with non-pregnant women or the general population. The result of a meta-analysis of 74 cohort and case-control studies showed that preterm delivery, maternal mortality, NICU admission and neonatal death in pregnant women with COVID-19 infection were significantly more than in those without COVID-19 infection.
This result is similar to the results of some meta-analyses performed. Karaçam et al. (Citation2022) based on the results of a meta-analysis of 54 studies, reported that morbidity, preterm and caesarean birth rates necessitating admission to the intensive care unit as well as maternal and perinatal death rates were higher in pregnant women with COVID-19 and their infants (Karaçam et al. Citation2022). As Jafari et al. (Citation2021) showed that preterm birth, caesarean delivery and LBW were more probable in women with COVID-19 compared to women without COVID-19 (Jafari et al. Citation2021). Gao et al. (Citation2020) also reported that the rate of preterm labour in healthy pregnant women worldwide is lower than that in pregnant women with COVID-19. They believe that the probable reason for this higher rate is the higher rate of induction in women with COVID-19 in the third trimester of pregnancy. Most of these women also choose to give birth prematurely by caesarean section to prevent prolonged labour (Gao et al. Citation2020).
Our study showed that pregnancy loss and SARS-CoV2 positive neonates in lower middle income were higher than in high income. Consistent with this result, a meta-analysis by Yang et al. (Citation2022) comparing pandemic and pre-pandemic periods showed that stillbirths were higher for middle-income countries but not for high-income countries (Yang et al. Citation2022).
The current systematic review showed that the most common signs and symptoms of pregnant women were fever, dry cough and fatigue. However, other less common symptoms, including headache, myalgia, nasal congestion, sore throat, dyspnoea, chills, body aches, conjunctivitis, skin rash, diarrhoea, loss of taste or smell, and discolouration of fingers or toes, have been reported (Hassanipour et al. Citation2020, Khan et al. Citation2020, Berghella and Hughes Citation2021, Saadaoui et al. Citation2021). In pregnant women, as in other adults, fever was a common clinical manifestation at the onset of COVID-19. Evidence has shown that intrapartum fever may lead to adverse neonatal outcomes (Dior et al. Citation2016). Jafari et al. (Citation2021) based on a meta-analysis reported that pregnant women with COVID-19 had similar clinical, laboratory and imaging characteristics to non-pregnant adult patients in the general population (Jafari et al. Citation2021). A systematic review and meta-analysis found that being symptomatically varied across ethnicities, with black and Asian pregnant women more likely to be symptomatic, while white pregnant women were more likely to be asymptomatic (Khan et al. Citation2021).
Pregnant women are more susceptible to respiratory pathogens and pneumonia due to the immunosuppressive state as well as physiological differences which often lead to severe hypoxia (O'Day Citation1997, Ramsey and Ramin Citation2001, Mosby et al. Citation2011, Mertz et al. Citation2013, Chen et al. Citation2020, Liu et al. Citation2020a, Citation2020c). Therefore, infection with the COVID-19 during pregnancy is expected to increase the risk of maternal and foetal complications, and women with severe pneumonia to be more at risk for adverse pregnancy outcomes. But the results of different studies about the adverse pregnancy outcomes in women infected with COVID-19 were very different.
The comparison of the outcomes in patients with or without COVID-19 in analytical studies showed that some of the feto-maternal outcomes such as preterm birth (Marín Gabriel et al. Citation2020, Abedzadeh‐Kalahroudi et al. Citation2021, Chinn et al. Citation2021, Cruz Melguizo et al. Citation2021, Gupta et al. Citation2021, Katz et al. Citation2021, Milln et al. Citation2021, Taghavi et al. Citation2021, Timircan et al. Citation2021), PROM (Cruz-Lemini et al. Citation2021, Cruz Melguizo et al. Citation2021, Du et al. Citation2021, Timircan et al. Citation2021), PPROM (Cruz Melguizo et al. Citation2021), GDM (Ko et al. Citation2021), gestational hypertension (Ko et al. Citation2021), pre-eclampsia/eclampsia (Abedzadeh‐Kalahroudi et al. Citation2021, Cruz Melguizo et al. Citation2021, Ko et al. Citation2021, Wilk et al. Citation2021), foetal distress (Abedzadeh‐Kalahroudi et al. Citation2021, Gupta et al. Citation2021), stillbirth (Cruz Melguizo et al. Citation2021), pregnancy morbidity (Tadas et al. Citation2021), IUFD (Hcini et al. Citation2021), PPH (Hcini et al. Citation2021), maternal mortality (Chinn et al. Citation2021), and prolonged labour (Wilk et al. Citation2021) in pregnant women with Covid-19 were significantly more than in those without Covid.
The function of the immune system in pregnant women is very complex. Therefore, maternal and neonatal outcomes will be different in each pregnant woman based on gestational age, immune system, duration of infection, and severity of infection (Banaei et al. Citation2020).
There are different opinions about changes in the immune response in pregnant women. Some have suggested that the transition to a Th2 anti-inflammatory environment during pregnancy may result in protection from a severe COVID-19 presentation (Dashraath et al. Citation2020, Saadaoui et al. Citation2021). It has also been reported that COVID-19 infection during pregnancy was characterised by placental inflammation and reduced antiviral antibody responses, which may impact the efficacy of COVID-19 therapeutics in pregnancy (Sherer et al. Citation2020). In our systematic review, maternal mortality was uncommon. This result is consistent with the results of other review studies (Allotey et al. Citation2020, Khalil et al. Citation2020, Lassi et al. Citation2021, Saadaoui et al. Citation2021).
COVID-19 may be associated with some neonatal outcomes. Based on the comparison of the outcomes in patients with or without COVID-19 in analytical studies, the main adverse neonatal outcome found is iatrogenic preterm birth (Timircan et al. Citation2021), and neonatal or NICU admission (Cruz-Lemini et al. Citation2021, Cruz Melguizo et al. Citation2021, Milln et al. Citation2021). There is no evidence for congenital malformations associated with maternal infection.
Some studies showed that women with pneumonia during pregnancy were more likely to have preterm deliveries, LBW and SGA infants than women without pneumonia (Bánhidy et al. Citation2008, Brito and Niederman Citation2011, Romanyuk et al. Citation2011, Chen et al. Citation2012). Some studies have also reported that SARS during pregnancy is associated with high incidences of spontaneous miscarriage, preterm delivery and intrauterine growth restriction (Wong et al. Citation2004).
This finding is consistent with other review studies that reported that preterm delivery, foetal distress and LBW were the common pregnancy outcomes of women with COVID-19 (Banaei et al. Citation2020, Mullins et al. Citation2020, Mark et al. Citation2021).
A systematic review and meta-analysis to evaluate differences in pregnancy and perinatal outcomes among symptoms compared with asymptomatic pregnant women infected with COVID-19 showed that the mean birth weight was significantly lower, while the probability of LBW and preterm delivery was more common among symptomatic pregnant women (Khan et al. Citation2021). Another systematic study reported that preterm delivery before 37 weeks of gestation was common in 21.8% of pregnant women with COVID-19 (Khalil et al. Citation2020).
The possibility of vertical transmission of COVID-19 is a tremendous concern for both patients and neonatologists and neonatal health care providers. Information on vertical transmission of COVID-19 is limited in studies and there is controversial information about the vertical transmission of COVID-19. In our systematic review, 32 studies reported the number of positive newborns for COVID-19, which may indicate vertical transmission from mother to foetus or due to infection after birth and it is not clear whether the source of the reported infection in these neonates is from the mother or from the environment. Our meta-analysis showed that there were SARS-CoV2 positive in 2% of infected mothers neonates.
Wang et al. (Citation2020) summarised that there is currently no evidence of intrauterine infection due to vertical transmission in women with COVID-19 in the third trimester of pregnancy, but it is unclear whether COVID-19 infection in the first or second trimester of pregnancy can carry the risk of vertical transmission or not? (Wang et al. Citation2020). Musa et al. (Citation2021) based on a review of 69 studies, reported that most of the mother-to-child infection was likely due to environmental exposure, although a significant proportion was attributable to potential vertical transmission of SARS-CoV-2 (Musa et al. Citation2021).
However, in the majority of studies, there was no evidence of vertical transmission and the findings of some systematic reviews do not also support the possibility of vertical transmission of COVID-19 infection (Banaei et al. Citation2020, Islam et al. Citation2020, Mullins et al. Citation2020). The results of some meta-analyses also showed that the possibility of vertical transmission from mother to foetus is low (Jafari et al. Citation2021, Kotlyar et al. Citation2021). Current evidence suggests that neonates and children do not develop severe COVID-19, and neonatal mortality is rare. However, we must be careful about the possibility of vertical transmission. It is important to diagnose neonatal infection because neonates can play a role in creating community-related infections (Saadaoui et al. Citation2021).
The current systematic review and meta-analysis have several strengths. First, we included in this systematic review 141 studies and conducted a meta-analysis of 74 studies with a large number of pregnant women that contribute to a more comprehensive understanding of COVID-19 in pregnancy. Second, we followed the correct methodology for conducting the present systematic review. Third, this study presents pregnancy outcomes of COVID-19 from different countries’ perspectives. The limitation of this study was the high heterogeneity in methods, study designs and estimates, which made meta-analysis difficult for all of them, so we performed a meta-analysis on cohort and case-control studies. Another limitation is that we were only able to search for articles in the PubMed and Scopus databases, and it was not possible for us to access other databases. Also, we only included English language articles in the study.
The findings of this study, as well as recently published systematic reviews and meta-analysis, may help physicians understand the nature of the disease and make appropriate decisions when treating pregnant women with COVID-19. Certainly, early identification and intervention of patients can reduce adverse pregnancy outcomes and improve the consequences of pregnancy. However, further studies are needed to confirm the long-term outcomes and potential vertical transmission from mother to foetus. On the other hand, with the identification of new strains of COVID-19, there are still questions as to whether each of these strains has more severe effects on the mother, foetus and newborn.
Conclusions
COVID-19 infection during pregnancy may cause adverse pregnancy outcomes including preterm delivery, maternal mortality, NICU admission and neonatal death. Pregnancy loss and SARS-CoV2 positive neonates in lower middle income are higher than in high income. The findings and knowledge gained from our systematic review show that the reported pregnancy outcomes for women with COVID-19 were been varied. Although studies reported some feto-maternal and neonatal outcomes, future studies are needed to elucidate the causal relationship between these outcomes and COVID-19 infection. Vertical transmission from mother to foetus may occur, but its immediate and long-term effects on the newborn are unclear. Therefore, due to the high transmission capacity of this virus, the treatment team should be aware of the possibility of vertical transmission and take the necessary measures and attention. Also, if the mother is seriously ill, separation from the newborn should be considered.
Supplemental Material
Download MS Word (7.4 MB)Acknowledgements
The authors thank all authors of the primary studies included in this review.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Data availability statement
All data relevant to the study are included in the article or uploaded as supplementary information. The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request.
References
- Abedzadeh‐Kalahroudi, M., et al., 2021. Maternal and neonatal outcomes of pregnant patients with COVID‐19: a prospective cohort study. International Journal of Gynaecology and Obstetrics, 153 (3), 449–456.
- Allotey, J., et al., 2020. Clinical manifestations, risk factors, and maternal and perinatal outcomes of coronavirus disease 2019 in pregnancy: living systematic review and meta-analysis. BMJ. 370:m3320.
- Ashish, K., et al., 2020. Effect of the COVID-19 pandemic response on intrapartum care, stillbirth, and neonatal mortality outcomes in Nepal: a prospective observational study. Lancet Global Health, 8, e1273–e1281.
- Banaei, M., et al., 2020. Obstetrics and neonatal outcomes in pregnant women with COVID-19: a systematic review. Iranian Journal of Public Health, 49 (Suppl. 1), 38–47.
- Bánhidy, F., et al., 2008. Maternal acute respiratory infectious diseases during pregnancy and birth outcomes. European Journal of Epidemiology, 23 (1), 29–35.
- Bank, T.W., 2021. The world by income and region [Online]. The World Bank. Available from: https://datatopics.worldbank.org/world-development-indicators/the-world-by-income-and-region.html [Accessed 19 Sep 2022].
- Berghella, V. and Hughes, B., 2021. COVID-19: pregnancy issues and antenatal care. Waltham, MA: UpToDate.
- Brito, V. and Niederman, M.S., 2011. Pneumonia complicating pregnancy. Clinics in Chest Medicine, 32 (1), 121–132.
- Cauldwell, M., et al., 2021. Seasonal and SARS‐CoV‐2 pandemic changes in the incidence of gestational diabetes. British Journal of Gynecology, 128 (11), 1881–1887.
- Chen, H., et al., 2020. Clinical characteristics and intrauterine vertical transmission potential of COVID-19 infection in nine pregnant women: a retrospective review of medical records. Lancet, 395 (10226), 809–815.
- Chen, Y.-H., et al., 2012. Pneumonia and pregnancy outcomes: a nationwide population-based study. American Journal of Obstetrics and Gynecology, 207 (4), 288.e1–288.e7.
- Chinn, J., et al., 2021. Characteristics and outcomes of women with COVID-19 giving birth at US academic centers during the COVID-19 pandemic. JAMA Network Open, 4 (8), e2120456.
- Cruz-Lemini, M., et al., 2021. Obstetric outcomes of SARS-CoV-2 infection in asymptomatic pregnant women. Viruses, 13 (1), 112.
- Cruz Melguizo, S., et al., 2021. Pregnancy outcomes and SARS-CoV-2 infection: the Spanish Obstetric Emergency Group Study. Viruses, 13 (5), 853.
- Dashraath, P., et al., 2020. Coronavirus disease 2019 (COVID-19) pandemic and pregnancy. American Journal of Obstetrics and Gynecology, 222 (6), 521–531.
- Dior, U.P., et al., 2016. Very high intrapartum fever in term pregnancies and adverse obstetric and neonatal outcomes. Neonatology, 109 (1), 62–68.
- Du, M., et al., 2021. Association between the COVID-19 pandemic and the risk for adverse pregnancy outcomes: a cohort study. BMJ Open, 11 (2), e047900.
- Gao, Y.J., et al., 2020. Clinical features and outcomes of pregnant women with COVID-19: a systematic review and meta-analysis. BMC Infectious Diseases, 20 (1), 564.
- Goyal, M., et al., 2021. The effect of the COVID‐19 pandemic on maternal health due to delay in seeking health care: experience from a tertiary center. International Journal of Gynaecology and Obstetrics, 152 (2), 231–235.
- Gupta, P., Kumar, S., and Sharma, S.S., 2021. SARS-CoV-2 prevalence and maternal–perinatal outcomes among pregnant women admitted for delivery: experience from COVID-19-dedicated maternity hospital in Jammu, Jammu and Kashmir (India). Journal of Medical Virology, 93 (9), 5505–5514.
- Hassanipour, S., et al., 2020. A systematic review and meta-analysis of pregnancy and COVID-19: signs and symptoms, laboratory tests, and perinatal outcomes. International Journal of Reproductive Biomedicine, 18 (12), 1005–1018.
- Hcini, N., et al., 2021. Maternal, fetal and neonatal outcomes of large series of SARS-CoV-2 positive pregnancies in peripartum period: a single-center prospective comparative study. European Journal of Obstetrics, Gynecology, and Reproductive Biology, 257, 11–18.
- Islam, M.M., et al., 2020. Clinical characteristics and neonatal outcomes of pregnant patients with COVID-19: a systematic review. Frontiers in Medicine, 7, 573468.
- Jafari, M., et al., 2021. Clinical characteristics and outcomes of pregnant women with COVID-19 and comparison with control patients: a systematic review and meta-analysis. Reviews in Medical Virology, 31 (5), 1–16.
- Justman, N., et al., 2020. Lockdown with a price: the impact of the COVID-19 pandemic on prenatal care and perinatal outcomes in a tertiary care center. Israel Medical Association Journal, 22, 533–537.
- Karaçam, Z., et al., 2022. Maternal and perinatal outcomes of pregnancy associated with COVID-19: systematic review and meta-analysis. European Journal of Midwifery, 6 (July), 1–22.
- Katz, D., et al., 2021. The Society for Obstetric Anesthesia and Perinatology (SOAP) COVID-19 Registry: an analysis of outcomes among pregnant women delivering during the initial SARS-CoV-2 outbreak in the United States. Anesthesia & Analgesia, 133 (2), 462–473.
- Khalil, A., et al., 2020. SARS-CoV-2 infection in pregnancy: a systematic review and meta-analysis of clinical features and pregnancy outcomes. EClinicalMedicine, 25, 100446.
- Khan, D.S.A., et al., 2021. Differences in pregnancy and perinatal outcomes among symptomatic versus asymptomatic COVID-19-infected pregnant women: a systematic review and meta-analysis. BMC Pregnancy and Childbirth, 21 (1), 14.
- Khan, M.M.A., et al., 2020. COVID-19 infection during pregnancy: a systematic review to summarize possible symptoms, treatments, and pregnancy outcomes. MedRxiv.
- Kirchengast, S. and Hartmann, B., 2021. Pregnancy outcome during the first COVID 19 lockdown in Vienna, Austria. International Journal of Environmental Research and Public Health, 18 (7), 3782.
- Ko, J.Y., et al., 2021. Adverse pregnancy outcomes, maternal complications, and severe illness among US delivery hospitalizations with and without a COVID-19 diagnosis. Clinical Infectious Diseases, 73 (Suppl. 1), S24–S31.
- Kotlyar, A.M., et al., 2021. Vertical transmission of coronavirus disease 2019: a systematic review and meta-analysis. American Journal of Obstetrics and Gynecology, 224 (1), 35–53.e3.
- Lassi, Z.S., et al., 2021. A systematic review and meta-analysis of data on pregnant women with confirmed COVID-19: clinical presentation, and pregnancy and perinatal outcomes based on COVID-19 severity. Journal of Global Health, 11, 05018.
- Liu, D., et al., 2020a. Pregnancy and perinatal outcomes of women with coronavirus disease (COVID-19) pneumonia: a preliminary analysis. American Journal of Roentgenology, 215 (1), 127–132.
- Liu, H., et al., 2020b. Why are pregnant women susceptible to COVID-19? An immunological viewpoint. Journal of Reproductive Immunology, 139, 103122.
- Liu, W., et al., 2020c. Coronavirus disease 2019 (COVID-19) during pregnancy: a case series.
- Lopes De Sousa, Á.F., et al., 2020. Effects of COVID-19 infection during pregnancy and neonatal prognosis: what is the evidence? International Journal of Environmental Research and Public Health, 17 (11), 4176.
- Marín Gabriel, M.A., et al., 2020. Maternal, perinatal and neonatal outcomes with COVID-19: a multicenter study of 242 pregnancies and their 248 infant newborns during their first month of life. Pediatric Infectious Disease Journal, 39 (12), e393–e397.
- Mark, E.G., et al., 2021. Coronavirus disease 2019 in pregnancy and outcomes among pregnant women and neonates: a literature review. Pediatric Infectious Disease Journal, 40 (5), 473–478.
- Mascarenhas, V.H.A., et al., 2020. COVID-19 and the production of knowledge regarding recommendations during pregnancy: a scoping review. Revista Latino-Americana de Enfermagem, 28, e3348.
- Mertz, D., et al., 2013. Populations at risk for severe or complicated influenza illness: systematic review and meta-analysis. British Medical Journal, 347 (1), f5061.
- Milln, J., et al., 2021. Clinical characteristics and pregnancy outcomes of women diagnosed with SARS-CoV-2 in London’s most ethnically diverse borough: a cross-sectional study. Obstetric Medicine, 14 (3), 164–169.
- Moher, D., et al., 2009. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of Internal Medicine, 151 (4), 264–269, w64.
- Mor, G., Aldo, P., and Alvero, A.B., 2017. The unique immunological and microbial aspects of pregnancy. Nature Reviews. Immunology, 17 (8), 469–482.
- Mosby, L.G., Rasmussen, S.A., and Jamieson, D.J., 2011. 2009 pandemic influenza A (H1N1) in pregnancy: a systematic review of the literature. American Journal of Obstetrics and Gynecology, 205 (1), 10–18.
- Mullins, E., et al., 2020. Coronavirus in pregnancy and delivery: rapid review. Ultrasound in Obstetrics & Gynecology, 55 (5), 586–592.
- Munn, Z., et al., 2019. The development of software to support multiple systematic review types: the Joanna Briggs Institute System for the Unified Management, Assessment and Review of Information (JBI SUMARI). JBI Evidence Implementation, 17, 36–43.
- Musa, S.S., et al., 2021. Vertical transmission of SARS-CoV-2: a systematic review of systematic reviews. Viruses, 13 (9), 1877.
- O'Day, M.P., 1997. Cardio-respiratory physiological adaptation of pregnancy. Seminars in Perinatology, 21 (4), 268–275.
- Ramsey, P.S. and Ramin, K.D., 2001. Pneumonia in pregnancy. Obstetrics and Gynecology Clinics of North America, 28 (3), 553–569.
- Ranjbar, F., et al., 2021. Changes in pregnancy outcomes during the COVID-19 lockdown in Iran. BMC Pregnancy and Childbirth, 21 (1), 1–6.
- Romanyuk, V., et al., 2011. Pneumonia during pregnancy: radiological characteristics, predisposing factors and pregnancy outcomes. Journal of Maternal-Fetal & Neonatal Medicine, 24 (1), 113–117.
- Rotshenker-Olshinka, K., et al., 2021. COVID-19 pandemic effect on early pregnancy: are miscarriage rates altered, in asymptomatic women? Archives of Gynecology and Obstetrics, 303 (3), 839–845.
- Saadaoui, M., Kumar, M., and Al Khodor, S., 2021. COVID-19 infection during pregnancy: risk of vertical transmission, fetal, and neonatal outcomes. Journal of Personalized Medicine, 11 (6), 483.
- Shakespeare, C., et al., 2021. Resilience and vulnerability of maternity services in Zimbabwe: a comparative analysis of the effect of Covid-19 and lockdown control measures on maternal and perinatal outcomes, a single-centre cross-sectional study at Mpilo Central Hospital. BMC Pregnancy and Childbirth, 21 (1), 1–8.
- Sherer, M.L., et al., 2020. Dysregulated immunity in SARS-CoV-2 infected pregnant women. medRxiv.
- Silva, C.R.A.C.D., et al., 2020. Immunological aspects of coronavirus disease during pregnancy: an integrative review. Revista da Associacao Medica Brasileira (1992), 66 (5), 696–700.
- Tadas, M., Prashanthi, S., and Waikar, M., 2021. Maternal and neonatal outcomes of pregnant women with covid-19: a case-control study at a tertiary care center in India. Journal of South Asian Federation of Obstetrics and Gynaecology, 13 (1), 44–49.
- Taghavi, S.-A., et al., 2021. Obstetric, maternal, and neonatal outcomes in COVID-19 compared to healthy pregnant women in Iran: a retrospective, case-control study. Middle East Fertility Society Journal, 26 (1), 1–8.
- Timircan, M., et al., 2021. Exploring pregnancy outcomes associated with SARS-CoV-2 infection. Medicina, 57 (8), 796.
- Wagner, M., et al., 2022. Perinatal and postpartum care during the COVID-19 pandemic: a nationwide cohort study. Birth, 49 (2), 243–252.
- Wang, C., et al., 2020. Intrauterine vertical transmission of SARS-CoV-2: what we know so far. Ultrasound in Obstetrics & Gynecology, 55 (6), 724–725.
- Wilk, M., et al., 2021. Diabetes management delivery and pregnancy outcomes in women with gestational diabetes mellitus during the first wave of the 2020 COVID-19 pandemic: a single-reference center report. Journal of Diabetes Research, 2021, 5515902.
- Wong, S.F., et al., 2004. Pregnancy and perinatal outcomes of women with severe acute respiratory syndrome. American Journal of Obstetrics and Gynecology, 191 (1), 292–297.
- World Health Organization, 2020. Global surveillance for COVID-19 disease caused by human infection with the 2019 novel coronavirus, interim guidance, 27 February 2020.
- Yang, J., et al., 2022. COVID-19 pandemic and population-level pregnancy and neonatal outcomes in general population: a living systematic review and meta-analysis (Update#2: November 20, 2021). Acta Obstetricia et Gynecologica Scandinavica, 101 (3), 273–292.
- Yu, N., et al., 2020. Clinical features and obstetric and neonatal outcomes of pregnant patients with COVID-19 in Wuhan, China: a retrospective, single-centre, descriptive study. Lancet Infectious Diseases, 20 (5), 559–564.
- Zaigham, M. and Andersson, O., 2020. Maternal and perinatal outcomes with COVID‐19: a systematic review of 108 pregnancies. Acta Obstetricia et Gynecologica Scandinavica, 99 (7), 823–829.