

Abstract
To describe predictors of patient satisfaction with pain control including opioid prescribing practices, patients undergoing minor gynaecologic and urogynaecologic surgeries were included in a prospective cohort study. Satisfaction with postoperative pain control by opioid prescription status was analysed using bivariate analysis and multivariable logistic regression, controlling for potential confounders. Among participants completing both postoperative surveys, 112/141 (79.4%) reported pain control satisfaction by day 1–2 and 118/137 (86.1%) by day 14. While we were underpowered to detect a true difference in satisfaction by opioid prescription, there were no differences in opioid prescription among patients satisfied with pain control [52% vs. 60% (p = .43) among satisfied patients at day 1–2 and 58.5% vs. 37% (p = .08) at day 14]. Significant predictors of pain control satisfaction were postoperative day (POD) 1–2 average pain at rest [aOR 0.72 (95% CI 0.52–0.99), p = .04], rating of shared decision-making [aOR 1.16 (95% CI 1.004–1.34), p = .04], amount of pain relief [aOR 1.28 (95% CI 1.07–1.54), p = .008) and POD 14 shared decision-making rating [aOR 1.45 (95% CI 1.19–1.77), p = .002].
What is already known on this subject? There are little data published on opioid prescription rates after minor gynaecologic procedures and no formal evidence-based guidance for gynaecologic providers for opioid prescribing. Few publications describe rates of opioid prescription and use following minor gynaecologic procedures. In the setting of a dramatic escalation of opioid misuse in the United States over the last decade, we sought to describe our practice of opioid prescription following minor gynaecologic procedures and answer the question of whether patient satisfaction is affected by opioid prescription, fill and use.
What do the results of this study add? Though underpowered to detect our primary outcome, our results suggest that patient satisfaction with pain control may primarily be significantly affected by the patient’s subjective assessment of shared decision-making with the gynaecologist.
What are the implications of these findings for clinical practice and/or further research? Ultimately, these preliminary findings suggest a larger cohort is needed to answer the question of whether pain control satisfaction is influenced by receipt/fill/use of opioids after minor gynaecologic surgery.
Impact Statement
Introduction
There has been a dramatic escalation in opioid prescriptions in the United States since the late 1990s (CDC Citation2011, 2017). Although the opioid prescription rate in the United States has been decreasing since 2012, the amount of opioid prescribed per person, quantified in morphine milligram equivalents (MMEs), has tripled since 1999 (CDC Citation2017). The 2019 National Survey on Drug Use and Health found that the majority of prescription misuse was associated with opioid-type drug prescriptions (Substance Abuse and Mental Health Services Administration Citation2019). The quantity of opioids prescribed is associated with long-term opioid use: Shah et al. (Citation2017) found a positive correlation between the number of days supplied in the first opioid prescription and probability of persistent 1- and 3-year opioid use.
These concerns should be pertinent to gynaecologists, as women may be particularly vulnerable to substance use disorders. Women undergo faster progression from initial use to opioid-related health problems and substance use disorder when compared to men (Moss et al. Citation2019). The severity and acuity of postoperative pain may contribute to persistent opioid use (As-Sanie et al. Citation2017, Johnson and Makai Citation2019). Thus, postoperative pain control must be balanced with the risks posed by excess opioids. Overprescribing opioid pain medication has likely contributed to opioid diversion with emerging literature suggesting postoperative patients commonly use less than half of what is prescribed (Johnson and Makai Citation2019).
There are no current evidence-based protocols to guide surgeons on appropriate opioid prescribing practices following gynaecologic surgeries, particularly after minor procedures. Additionally, minor gynaecologic surgeries are excluded from enhanced recovery after surgery (ERAS) protocols. We sought to describe predictors of patient satisfaction with pain control including opioid prescribing practices following minor gynaecologic surgery. We hypothesised that patient satisfaction would not be affected by receipt of postoperative opioid prescription.
Materials and methods
Study design and population
This study was conducted as a prospective observational study, approved by the Johns Hopkins Institutional Review Board (IRB #00194966, approved 12/2018) between September 2018 and May 2019. All patients undergoing outpatient gynaecologic surgeries at our hospital were eligible. Major surgery (hysterectomy, laparoscopic or open abdominal myomectomies, abdominal prolapse repairs) and pregnancy terminations were excluded. Minor gynaecologic surgeries were defined as diagnostic and operative hysteroscopies, combined hysteroscopy and laparoscopy, diagnostic and operative laparoscopies, sub-urethral sling placements, diagnostic and operative cystoscopies, vaginal prolapse repairs and ‘other’ minor procedures (Supplemental Table 2). Patients were also excluded if they were younger than 18, currently incarcerated (self-report), reported preoperative regular use of opioid medication (oxycodone, oxycodone/acetaminophen, codeine, fentanyl, hydrocodone, hydromorphone, methadone, morphine, oxymorphone, tramadol), a history of illicit substance use within the last 6 months prior to study entry, a history of chronic pelvic pain (defined as pelvic pain consistently present for 6 months or greater in duration), allergy or intolerance to ibuprofen or acetaminophen, if the planned procedure was performed in conjunction with another non-gynaecologic surgical service, or the patient was non-English speaking. STROBE guidelines for observational studies were followed in preparation of this study and manuscript (von Elm Citation2008).
Table 2. Patient satisfaction and postoperative characteristics by opioid prescription.
Chart abstraction was performed to confirm the performed procedure, anaesthesia time and type, operative difficulties and opioid prescription. Patients were surveyed preoperatively (within 1 week prior to surgery), on postoperative day (POD) 1 or 2 and finally at POD 14. Survey instruments were emailed to patients through Research Electronic Data Capture (REDCap) at Johns Hopkins University School of Medicine (Harris et al. Citation2009) and follow up phone calls were made by study personnel up to three times to assist with survey completion. Research Electronic Data Capture is a secure, web-based application designed to support data capture for research studies, providing: (1) an intuitive interface for validated data entry; (2) audit trails for tracking data manipulation and export procedures; (3) automated export procedures for seamless data downloads to common statistical packages; and (4) procedures for importing data from external sources.
The pre-operative survey included baseline symptoms (constipation, pruritus, difficulty sleeping, nausea and poor appetite/anorexia) and the Surgical Pain Scales (SPSs), which evaluates average pain at rest, with normal activities, and with more strenuous activities (Barber et al. Citation2012). Each domain is scored from 0 to 10, with 0 representing no pain. To assess pre-operative anxiety, we used the Beck Anxiety Index (BAI), which scores anxiety from 0 to 63 (scores 0–3 across 21 domains, with 0 representing no anxiety). Other covariates assessed by questionnaire prior to surgery included age, race, ethnicity, parity and educational attainment.
We then reviewed the electronic medical record to identify patients who received an opioid prescription. Postoperative day 1–2 results are referred to as ‘immediate’ while POD 14 results are ‘delayed’. Postoperative survey responses were used to determine the proportion of women who filled and used their opioid prescriptions and report total used at the POD 1–2 and by POD 14. We measured postoperative pain severity and pain during activities using the SPS and the International Pain Outcomes Questionnaire (IPO) (Rothaug et al. Citation2013), both completed on POD 1–2 and day 14. The IPO includes questions which evaluate a Numeric Rating Scale (NRS) for the worst pain and least pain since surgery, the frequency of time spent in severe pain, and a numeric rating of pain interference with certain activities (movement in bed, deep breathing or coughing, sleeping). Additional non-validated questions were added to questionnaires at both postoperative time points. Each participant was asked to estimate the percentage of pain relief from all pain treatments (medical and non-medical), whether the patient would have liked additional pain medication, and whether the patient received sufficient information about pain treatment options. In addition, each patient was asked to rate (how much they were allowed to participate in decisions about their pain treatment 0 = no participation, 10 = high participation) to assess their participation in shared decision making. Other covariates included age, race, ethnicity, parity and educational attainment (Supplementary Appendix).
The primary outcome for this study was satisfaction with postoperative pain control, defined by an NRS, with the question ‘Indicate one number that best shows how satisfied you are with the results of your pain treatment since your surgery’ (NRS, 0 = extremely dissatisfied, 10 = extremely satisfied) (Davidson et al. Citation2020, Fry et al. Citation2021). This outcome was dichotomised by those who were satisfied and those who were not satisfied with their pain control: patients who reported a score of >8 were classified as ‘satisfied’ with pain control based on skewed response distribution towards satisfaction and ease of comparison. Pain treatment satisfaction was reported at day 1–2 and day 14 and we report responses at both time points. Secondary outcomes of the study included describing opioid prescription practices by providers and fill and use practices by patients after minor gynaecologic surgery. Chart review was also performed to capture intraoperative parameters include total duration of anaesthesia time.
Sample size and statistical analysis
This study was designed as a preliminary investigation of the effect of opioid prescription on patient satisfaction after minor gynaecologic surgeries, thus a sample size of convenience was chosen for this study. We anticipated approximately 780 women undergoing all gynaecologic surgeries over a two-year period and estimated that 85% of participants would complete follow up surveys. To characterise women who were satisfied versus those who were dissatisfied with pain control, we considered survey results from both POD 1–2 and POD 14. At each time point, satisfaction with pain control was dichotomised as ‘satisfied’ with an NRS >8 and ‘non-satisfied’ as NRS ≤8, as the scores were not normally distributed. Characteristics were compared between those who were satisfied versus non-satisfied, using Fisher’s exact tests and Wilcoxon’s rank sum for categorical or continuous variables, respectively. Logistic regression modelling was used to examine the association between satisfaction with pain control and opioid prescription, adjusting for variables found to be significantly associated with pain control satisfaction in bivariate analysis. Standard model diagnostics were examined and variables with high correlation (>0.8) were excluded from the full model out of concern for collinearity. Additionally, goodness of fit was confirmed for all models. We report odds ratios with 95% confidence intervals. All data analyses were performed using SAS 9.4 (Cary, NC). A p value of ≤.05 was considered statistically significant. A post hoc power analysis was completed.
Results
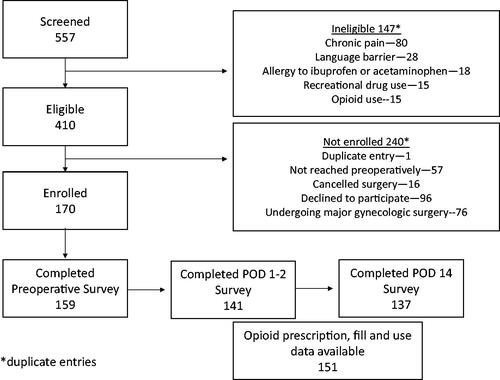
A total of 557 women undergoing gynaecologic surgery were screened between September 2018 and May 2019 and 170 were enrolled in this study (). One hundred and thirty-four (84.2%) of patients completed all surveys.
Figure 1. Enrollment Flow Diagram. Sums of categories containing duplicates may be higher than the total number of patients because patients may have been part of multiple categories.
There were no significant baseline or procedure-level differences associated with opioid prescribing (). However, women who received an opioid prescription had lower preoperative anxiety (median Beck Anxiety score 3 vs. 4, p=.05). Of the 81 women who received an opioid prescription, 68 (84%) filled the prescription and 55 of those (81%) reported using the opioid medication. Receipt of an opioid prescription was associated with delayed satisfaction with pain control though this did not reach statistical significance; 58.5% of satisfied patients and 37% of non-satisfied patients (p=.08) received an opioid prescription. Total anaesthesia time was longer among those who filled versus did not fill a prescribed opioid prescription (median 86 vs. 64 minutes, p=.03) (). Supplemental Table 1 outlines opioid prescription, fill and use data by procedure type.
Table 1. Demographics by opioid prescription status.
Among participants who completed post-operative surveys, 112/141 (79.4%) reported satisfaction with their pain control by day 1–2 and 118/137 (86.1%) respondents reported satisfaction with their postoperative pain control by day 14. Patients reporting immediate satisfaction with pain control (based on day 1–2 data, n = 112) had higher scores for postoperative shared decision-making over pain control (median score 11 vs. 4, p < .0001), and higher percent amount of pain relief (p=.0003) in bivariate analysis ( and Supplemental Table 2). Patients with immediate pain control satisfaction also reported less frequent desire for additional pain medications (2.7% vs. 38%, p<.0001) and were more likely to report receipt of sufficient pain treatment information (p=.02). In logistic regression modelling, significant predictors of immediate pain control satisfaction were the POD1–2 average pain at rest (adjusted OR 0.72 (95% CI 0.52–0.99), p=.04), rating of shared decision-making over pain control (aOR 1.16 (95% CI 1.004–1.34), p=.04) and percent amount of pain relief (aOR 1.28 (95% CI 1.07–1.54), p=.008) after adjustment for rating of disturbance of average pain, total constipation and insomnia scores, frequency of time spent in severe pain, pain interference with activities and adequate provision of pain treatment information ().
Table 3. Factors examined in logistic regression analysis predicting immediate and delayed satisfaction with pain control.
Patients reporting satisfaction with pain control by day 14 (n = 118) were younger (mean age 49.0 vs. 58.4, p=.01), without other differences in demographics ( and Supplemental Table 3). Patients satisfied with pain control by day 14 reported high shared decision-making scores (median 10 vs. 0, p<.0001), but higher postoperative anxiety (median BAI score 43 vs. 29, p<.0001). Patients who were not satisfied with delayed postoperative pain control more frequently reported a desire for additional pain medications (26.3% vs. 0.85%, p<.0001) and less frequently reported that sufficient pain treatment information had been provided (52.6% vs. 71.2%, p=.02). In logistic regression modelling for day 14 pain satisfaction, pain satisfaction was best predicted by shared decision-making rating (aOR 1.45 (95% CI 1.19–1.77), p=.002) after adjustment for age, day 14 frequency of time spent in severe pain, percent amount pain relief, day 14 nausea intensity, preoperative average pain at rest score, preoperative perception of amount of pain with exercise and preoperative perception of worst pain rating ().
In exploratory sub-group analyses, we compared patients undergoing laparoscopic procedures versus vaginal surgeries (all non-laparoscopic procedures included). Among the 14 patients who had any laparoscopic procedure 12/14 (85.7%) were prescribed opioids compared to 64/127 (50.4%) of the non-laparoscopic procedures (p=.009). Despite this, there was no difference in pain satisfaction at POD 1–2 (9/13 [69.2%] patients who had laparoscopy were satisfied vs. 77/98 [78.6%] patients who had non-laparoscopic procedure, p = .19) and at POD 14 (14/14 patients who had laparoscopy were satisfied vs. 104/123 (84.6%) patients who had non-laparoscopic procedure, p = .11).
Discussion
After minor gynaecologic surgery, approximately half of surveyed patients received a prescription for postoperative opioids, and among patients receiving an opioid prescription, 68% of women filled and reported use. While our preliminary results suggest that opioid prescription was not associated with postoperative satisfaction with pain control, it will be important to validate this study in a larger cohort to verify or refute that opioid prescription after minor gynaecologic surgery may not be required for most patients for adequate pain management. Shared decision-making with patients and subjective assessment of sufficient pain treatment information appear to be critical components of postoperative pain satisfaction. In our study, 58.5% of satisfied patients and 37% of non-satisfied patients (p=.08) received an opioid prescription. Though this difference did not reach statistical significance likely due to insufficient patient number, a 21.5% absolute risk difference suggests that opioid prescriptions were issued more often in the satisfied cohort. Additionally, on day 14 surveys, patients who were not satisfied with their pain control reported a desire for additional medications and felt that pain treatment information was inadequate more frequently than those reporting pain control satisfaction.
Opioid prescribing following minor gynaecologic procedures happens more frequently than one might imagine despite lacking guidance on appropriate prescribing practices by procedure type. Wright et al. reported that 36.7% of patients received an opioid prescription following dilation and curettage, and authors were concerned for new persistent opioid use after such prescriptions (Wright et al. Citation2019). Griffith et al. (Citation2018) reported that in an online survey of 51 physicians, 40% provide opioids after a hysteroscopic procedure and 19.2% following a dilation and curettage. In the same survey, 64.6% of 56 responding patients used less than half of the opioids prescribed and 16.1% used none. Moss et al. (Citation2021) report regional variations in opioid prescribing practices following hysteroscopic procedures. Similarly, Patanwala et al. (Citation2020) reported that a cohort of gynaecologic surgeons performing minor laparoscopies and major gynaecologic surgery (via laparotomy or minimally invasively), prescribed almost three times more opioid tablets and MMEs than were used by patients without an effect on reported pain levels. Consistent with these data, we found a significant discrepancy between opioid prescription and use, particularly after diagnostic procedures. Our data primarily suggest that gynaecologic surgeons should involve patients in discussions about their planned postoperative pain control, as shared decision-making influenced longer term pain control satisfaction. Shared decision making to reduce opioid prescribing following hysterectomy has been described by Vilkins et al. (Citation2019).
Overall, besides changing individual provider opioid prescribing practices, systemic interventions are needed to help reduce postoperative opioid prescribing. Some examples of systemic changes include state level legislation mandating a decrease (Carrubba et al. Citation2021), adjusting default prescribing thresholds in electronic medical records (Chiu et al. Citation2018) and adopting restrictive opioid prescribing policies (Mark et al. Citation2018). In a recent randomised controlled trial, Plewniak et al. allocated 120 women scheduled for minor gynaecologic laparoscopy to standard tablet or low tablet number opioid prescribing after surgery. The primary outcome was the number of oxycodone tablets used by days 1 and 7. The authors found that the median number of oxycodone tablets did not differ by day 7 and that most patients reported taking three or fewer tablets by that timepoint (Plewniak et al. Citation2021). Over time, one group identified decreasing trends in opioid prescribing following laparoscopic sterilisations but highlight the need for evidence-based approaches to inform postoperative opioid prescribing practices (Arabkhazaeli et al. Citation2021). Additional interventions reported include use of multi-modal anaesthesia intraoperatively. Low dose spinal anaesthesia in combination with general anaesthesia reduced perioperative opioid consumption in laparoscopic gynaecologic surgery in the immediate postoperative period (Zdravkovic and Kamenik Citation2020).
To the best of our knowledge, few studies have investigated the impact on opioid prescription following gynaecologic surgery on patient satisfaction. Davidson et al. (Citation2020) published a randomised controlled noninferiority trial of reduced versus routine opioid prescription after prolapse repair with a primary objective of comparing patient satisfaction by opioid prescription group after prolapse repair. One hundred and sixteen patients were included. The difference between groups demonstrated noninferiority though patients in the reduced prescription group required additional opioid more frequently (15% vs. 2%, p=.01) and patients in the routine arm used more opioids than those in reduced arm (Davidson et al. Citation2020). Fry et al. (Citation2021) report on outcomes from a prospective cohort study evaluating opioid naïve adults undergoing laparoscopic cholecystectomy, laparoscopic appendectomy and minor hernia repair. The primary outcome was patient satisfaction. After multivariable adjustment, the authors found no significant association between opioid prescription size and satisfaction (OR 1.00, 95% CI 0.99–1.00). The predicted probability of being highly satisfied ranged from 83% for the smallest prescription (25 mg OME) to 85% for the largest prescription (750 mg OME) (Fry et al. Citation2021).
Strengths of this study include the prospective design and the inclusion of a broad variety of minor procedures. We acknowledge several limitations in our study design. The heterogeneity in surgery type may make it difficult to draw firm conclusions about less frequently performed or represented procedures. In addition, our results may not be completely generalisable to all women undergoing minor gynaecologic procedures because the patient population surveyed was undergoing surgery at a tertiary care centre and was limited to English speakers. Further, although the difference in opioid prescriptions between the satisfied and unsatisfied groups in at both measured time points was not significant, our post hoc power analysis revealed that we were under-powered to detect a difference; at POD 1–2 we would have needed a sample size of 1715 patients and at POD 14, 260 patients, to achieve 80% power to detect a difference in opioid prescriptions with the current proportion of satisfied to unsatisfied patients (4:1). The authors recognise that some patients still had pain despite opioid prescription, and some patients without prescription were less satisfied with their pain control. Given the detection of significant difference between groups was limited by underpowered sample size, the authors support continuing an individualised approach towards opioid prescription after minor gynaecologic surgery. Additional limitations include non-standardised intraoperative opioid use by anaesthesia providers and the inability to describe the MME patients received during their surgery in relation to pain or satisfaction postoperatively, particularly given intraoperative practices may have a significant effect on postoperative analgesic needs and satisfaction. Lastly, our final survey tool was not validated before our study and thus conclusions based on the data obtained from this item must be more guarded.
Ultimately, we hope this study will help guide additional studies needed to inform clinical decision making in determining the need for postoperative opioid prescribing following minor gynaecologic surgeries. Future studies should include a larger sample size to be adequately powered to detect differences in pain satisfaction by opioid prescription status and consider including women with chronic pelvic pain, as evidence is lacking on how best to manage their postoperative pain.
Author contributions
Study design – CM, AP, MB and VH; study participant recruitment – CM, CB and PP; statistics and AP; manuscript preparation – AP, CM, VH, MB and MM.
Supplemental Material
Download Zip (108.9 KB)Acknowledgements
The authors wish to thank the Johns Hopkins School of Medicine Biostatistics, Epidemiology and Data Management (BEAD) Core for assistance with statistical planning and analysis overview.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Additional information
Funding
References
- Arabkhazaeli, M., et al., 2021. Trends in opioid prescriptions after laparoscopic sterilization. Journal of the Society of Laparoscopic & Robotic Surgeons, 25 (1), e2020.00088.
- As-Sanie, S., et al., 2017. Opioid prescribing patterns, patient use, and postoperative pain after hysterectomy for benign indications. Obstetrics and Gynecology, 130 (6), 1261–1268.
- Barber, M.D., et al., 2012. Validation of the Surgical Pain Scales in women undergoing pelvic reconstructive surgery. Female Pelvic Medicine & Reconstructive Surgery, 18 (4), 198–204.
- [CDC] Centers for Disease Control and Prevention, 2011. Vital signs: overdoses of prescription opioid pain relievers – United States, 1999–2008. Morbidity and Mortality Weekly Report, 60, 1487–1492.
- [CDC] Centers for Disease Control and Prevention, 2017. Vital signs: changes in opioid prescribing in the United States, 2006–2015. Morbidity and Mortality Weekly Report, 66, 697–704.
- Carrubba, A.R., et al., 2021. Impact of legislation on opioid prescribing following hysterectomy and hysteroscopy in Arizona and Florida. Gynecologic and Obstetric Investigation, 86 (5), 460–468.
- Chiu, A.S., et al., 2018. Association of lowering default pill counts in electronic medical record systems with postoperative opioid prescribing. JAMA Surgery, 153 (11), 1012–1019.
- Davidson, E.R.W., et al., 2020. A randomized controlled noninferiority trial of reduced vs routine opioid prescription after prolapse repair. American Journal of Obstetrics and Gynecology, 223 (4), 547.e1–547.e12.
- Fry, B.T., et al., 2021. Association of postoperative opioid prescription size and patient satisfaction. Annals of Surgery, 276 (6), e1064–e1069.
- Griffith, K.C., et al., 2018. Opioid prescription and patient use after gynecologic procedures: a survey of patients and providers. Journal of Minimally Invasive Gynecology, 25 (4), 684–688.
- Harris, P.A., et al., 2009. Research Electronic Data Capture (REDCap) – a metadata-driven methodology and workflow process for providing translational research informatics support. Journal of Biomedical Informatics, 42 (2), 377–381.
- Johnson, C.M. and Makai, G.E.H., 2019. A systematic review of perioperative opioid management for minimally invasive hysterectomy. Journal of Minimally Invasive Gynecology, 26 (2), 233–243.
- Mark, J., et al., 2018. Ultrarestrictive opioid prescription protocol for pain management after gynecologic and abdominal surgery. JAMA Network Open, 1 (8), e185452.
- Moss, C., et al., 2019. Weaning from long-term opioid therapy. Clinical Obstetrics and Gynecology, 62 (1), 98–109.
- Moss, C.F., et al., 2021. Opioid dispensing after hysteroscopy in the United States. Obstetrics and Gynecology, 138 (6), 888–890.
- Rothaug, J., et al., 2013. Patients’ perception of postoperative pain management: validation of the International Pain Outcomes (IPO) Questionnaire. Journal of Pain, 14 (11), 1361–1370.
- Patanwala, I., et al., 2020. Opioid prescription usage after benign gynecologic surgery: a prospective cohort study. Journal of Minimally Invasive Gynecology, 27 (4), 860–867.
- Plewniak, K.M., et al., 2021. Examining reduced opioid prescriptions after gynecologic laparoscopy: a randomized controlled trial. Journal of Minimally Invasive Gynecology, 28 (2), 366–373.
- Shah, A., Hayes, C.J., and Martin, B.C., 2017. Factors influencing long-term opioid use among opioid naive patients: an examination of initial prescription characteristics and pain etiologies. Journal of Pain, 18 (11), 1374–1383.
- Substance Abuse and Mental Health Services Administration. 2019. Key substance use and mental health indicators in the United States: results from the 2019 National Survey on Drug Use and Health (HHS Publication No. PEP20-07-01-001, NSDUH Series H-55). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration.
- Vilkins, A.L., et al., 2019. Effects of shared decision making on opioid prescribing after hysterectomy. Obstetrics and Gynecology, 134 (4), 823–833.
- Von Elm, E., et al., 2008. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. Journal of Clinical Epidemiology, 61 (4), 344–349.
- Wright, J.D., et al., 2019. Use and misuse of opioids after gynecologic surgical procedures. Obstetrics and Gynecology, 134 (2), 250–260.
- Zdravkovic, M. and Kamenik, M., 2020. A prospective randomized controlled study of combined spinal-general anesthesia vs. general anesthesia for laparoscopic gynecological surgery: opioid sparing properties. Journal of Clinical Anesthesia, 64, 109808.